



{kind=link}


2 Minute Medicine Rewind August 7, 2017
Angiotensin II for the treatment of vasodilatory shock
Vasodilatory shock, characterized by decreased blood pressure despite adequate cardiac output, can progress to irreversible organ failure. Vasodilatory shock that does not respond to the use of high-dose vasopressors is associated with high mortality. While 2 major classes of vasopressors are generally used, including catecholamines and vasopressin, the renin-angiotensin-aldosterone system (RAAS) is also physiologically activated under these circumstances in an attempt to raise blood pressure. Previous studies have shown that modified bovine angiotensin II can elicit consistent vasopressor effects in patients with shock. In this randomized controlled trial, 344 patients with vasodilatory shock who were receiving over 0.2ug/kg/minute of norepinephrine or the equivalent dose of another vasopressor, were randomized to receive infusions of either angiotensin II or placebo, in order to determine whether the use of angiotensin II results in improvements in blood pressure. A response to angiotensin II was defined as an increase from baseline of at least 10 mmHg or an increase to at least 75 mm Hg at 3 hours, without an increase in the dose of background vasopressors. Researchers found that more patients in the angiotensin II group than in the placebo group met criteria for the primary endpoint of response (69.9% vs. 23.4%, OR 7.95, 95% CI 4.76 to 13.3, p<0.001). At 48 hours, the mean improvement in the cardiovascular Sequential Organ Failure Assessment (SOFA) score was also significantly greater in the angiotensin II group p=0.01), however, there were no significant differences in other SOFA score components. At 28 days of follow-up, there was no significant difference in mortality rate (HR 0.78, 95% CI 0.57 to 1.07, p=0.12). This study therefore shows that angiotensin II can effectively increase blood pressure in patients with vasodilatory shock with poor response to high doses of conventional vasopressors.
Immunoglobulin A nephropathy (IgA) is one of the most common primary glomerular diseases, with up to 30% of people affected by IgA nephropathy developing end-stage renal disease (ESRD). Renin-angiotensin-aldosterone system (RAAS) blockade has been shown to reduce the risk of renal failure in patients at particularly high risk of ESRD, including those with decreased kidney function, persistent proteinuria and hypertension. The use of immunosuppressants, on the other hand, has been controversial. In this randomized controlled trial, 262 patients with proteinuria >1 g/day and estimated glomerular filtrate rate (eGFR) of 20-120mL/min/1.73m2 and at least 3 months of blood pressure control were randomized to receive oral methylprednisolone (0.6-0.8 mg/kg/day) or matching placebo for 2 months to evaluate the efficacy and safety of corticosteroids in patients with IgA nephropathy. The primary composite end point was defined as the first occurrence of a 50% decrease in eGFR, the development of ESRD, or death due to kidney disease. Researchers found that patients in the intervention group were less likely to exhibit progression in their renal disease (HR 0.37, 95% CI 0.17 to 0.85, p=0.02). However, serious adverse events (SAEs) were more likely to occur in these patients compared to placebo (RR 4.63, 95% CI 1.63 to 13.2, p=0.001). This was mainly driven by an excess of serious infections among 11 patients (8.1%) in the intervention group, compared to no serious infections in the placebo group (risk difference 8.1%, 95% CI 3.5% to 13.9%, p<0.001). This study therefore shows that, while immunosuppression may provide some renal benefit to patients with IgA nephropathy and associated proteinuria, oral methylprednisolone is associated with an increased risk of serious adverse events, namely infections, bringing into question the safety of this immunosuppressive treatments.
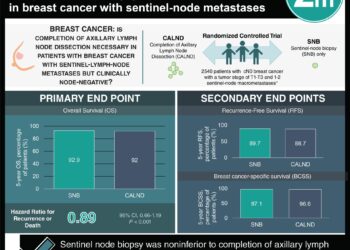
Breast-conserving surgery (BCS) results in lower complication rates, improved quality of life and equivalent or better survival rates when compared to mastectomy in patients with early stage breast cancer. However, some women require repeated surgery to increase resection margins, and as such, may not realize these benefits. In addition, the costs and complications resulting from additional surgery are not well characterized. In this retrospective study, insurance claims for 9,837 women that underwent BCS for breast carcinoma were reviewed to assess clinical complications and economic outcomes. Researchers found that 2,282 (23.3%, 95% CI 22.4% to 24.0%) of the study population underwent at least 1 additional breast operation. In the 3 months following the initial BCS, complications were twice as likely in patients undergoing a repeated breast surgery (p<0.001). Researchers also found that the mean cost for a patient undergoing any repeated surgery was 16,072 USD higher, with 56.4% of added costs being incurred within 6 months of the initial BCS. The mean 2-year total healthcare costs increased by 11,621 USD for patients undergoing a repeated BCS and 26,276 USD for patients undergoing a subsequent mastectomy. Overall, increased costs owing to a repeated surgery were statistically significant (p<0.001). This study therefore shows that there are considerable costs and risks of complication associated with surgery subsequent to BCS. This has important implications in advancing margin evaluation.
Exenatide is a glucagon-like peptide-1 (GLP-1) receptor agonist that has shown to have neuroprotective effects in preclinical models of Parkinson’s disease. At doses similar to that used in type 2 diabetes, it is able to cross the blood-brain barrier, exerting neuroprotective and neurorestorative effects via GLP-1 receptors, resulting in improvements in motor performance, behaviour, learning and memory. In this randomized controlled trial, 62 patients were randomly assigned to receive subcutaneous injections of exenatide 2 mg or placebo once weekly for 48 weeks, followed by a 12-week washout period, to assess effects of this drug on the motor severity of Parkinson’s disease. The primary outcome was change in the Movement Disorder Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part 3 scores in the practically defined off-medication state at 60 weeks. Researchers found that at 60 weeks of follow-up, MDS-UPDRS part 3 had worsened by 2.1 points (95% CI -0.6 to 4.8) in the placebo group and improved by 1.0 points (95% CI -2.6 to 0.7) in the exenatide group (p=0.0318). At 48 weeks, scores in the placebo group had decreased by 1.7 points (95% CI -0.6 to 4.0), and those in the intervention group had improved by 2.3 points (95% CI -4.1 to -0.7) (p=0.0026). This study therefore shows that exenatide had positive effects on off-medication motor scores in Parkinson’s disease, sustained beyond the period of exposure.
The prescription of opioid analgesics in the US has increased by more than 3-fold over the past 2 decades. Up to 22% of pregnancies in the US are complicated by exposure to prescription opioid medications. Neonatal abstinence syndrome (NAS) may result from intrauterine exposure to opioid analgesics, with neonates presenting with a variety of symptoms including difficulties with feeding and sleeping, impaired thermoregulation, seizures, failure to thrive and respiratory distress. Psychotropic medication exposure can also result in withdrawal signs; it is often difficult to ascertain whether signs of withdrawal are primarily the result of intrauterine exposure to opioids, psychotropic medications, or both. In this retrospective cohort study, 201,275 pregnant women exposed to opioids and/or psychotropic medications around the time of delivery were followed up to assess whether the risk of neonatal drug withdrawal in newborns exposed in utero is greater and more severe than in those exposed to opioid analgesics alone. Researchers found that among the 201,275 women exposed to prescription opioids in the 45 days prior to delivery, 7.0% also filled a prescription for an antidepressant, 0.5% for an antipsychotic, 2.7% for a benzodiazepine, 0.3% for gabapentin, and 5.0% for a Z-drug. The risk of withdrawal was increased among patients using antidepressants (RR 1.34, 95% CI 1.22 to 1.47), benzodiazepines (RR 1.49, 95% CI 1.35 to 1.63), and gabapentin (RR 1.61, 95% CI 1.26 to 2.06). Exposure to any single additional psychotropic medication (antidepressants, benzodiazepines or gabapentin) was associated with a 37% increased risk of withdrawal (RR 1.37, 95% CI 1.26 to 1.49). Exposure to 2 or more of these medications was associated with a doubling of this risk (RR 2.05, 95% CI 1.77 to 2.37). This study therefore shows that the use of psychotropic medications in addition to prescription opioids is not only common, but may also be associated with increased risk and severity of neonatal drug withdrawal.
Image: PD
©2017 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
