




{kind=link}


2 Minute Medicine Rewind June 26, 2017
First-line nivolumab in stage IV or recurrent non-small-cell lung cancer
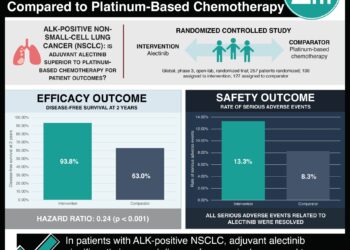
Platinum-based combination chemotherapy has long been used in the first-line treatment of patients with advanced non-small-cell lung cancer (NSCLC). However, chemotherapy only provides moderate benefit, with median progression-free survival and overall survival limited to 4-6 months and 10-13 months, respectively. Recent research has shown that nivolumab, a programmed death 1 (PD-1) immune-checkpoint-inhibitor antibody is associated with longer overall survival than docetaxel chemotherapy among patients with previously treated NSCLC. In this randomized controlled trial, 530 patients with untreated stage IV or recurrent NSCLC and a PD-L1 tumour expression level of 1% or more were randomized to receive nivolumab or platinum-based chemotherapy to study the efficacy and safety of nivolumab. Nivolumab was administered intravenously (3 mg/kg) every 2 weeks. Platinum-based chemotherapy was administered once every 3 weeks for up to 6 cycles. Researchers found that among patients with a PD-L1 expression level of 5% or more, there was no significant difference in progression-free survival (HR 1.15, 95% CI 0.91 to 1.45, p=0.25) or overall survival (HR 1.02, 95% CI 0.80 to 1.30) between treatment groups. Nivolumab did, however, have a favorable safety profile as treatment-related adverse events of any grade occurred in 71% of patients in the intervention group as compared to 92% of patients that had received chemotherapy. This study therefore shows that in patients with previously untreated stage IV or recurrent NSCLC with PD-L1 expression, nivolumab is not associated with significantly greater progression-free survival or overall survival when compared to conventional platinum-based chemotherapy.
Medications including beta-blockers, statins, aspirin and other antiplatelets significantly reduce the rate of cardiovascular events and need for repeated treatment procedures among patients surviving acute myocardial infarction (AMI). However, medication compliance remains poor. Wireless technology and behavioral economic approaches have shown promise in improving health behaviours. In this randomized controlled trial, 1503 AMI survivors were randomized to participate in an intervention using electronic pill bottles combined with lottery incentives and social support for medication adherence or usual care to determine whether a system of medication reminders using financial incentives and social support delays subsequent cardiovascular events following AMI. Researchers found that there was no statistically significant difference between treatment arms in terms of time to first readmission for a vascular event or death (HR 1.04, 95% CI 0.71 to 1.52, p=0.84) or time to first all-cause readmission (HR 0.89, 95% CI 0.73 to 1.09, p=0.27). There were also no significant differences in mean medication adherence between the control and intervention groups using strict (p=0.10) or relaxed (p=0.63) criteria. As such, the authors concluded that this compound intervention integrating wireless pill bottles, lottery-based incentives and social support did not improve medication adherence or vascular readmission outcomes.
Yoga, physical therapy or education for chronic low back pain: a randomized noninferiority trial
Lower back pain is the leading cause of disability worldwide. Physical therapy (PT) is the most common, evidence-based non-pharmacologic referral made by physicians for chronic lower back pain (cLBP). However, meta-analyses and several large randomized controlled trials have also supported the role of yoga in the management of cLBP. In this randomized controlled trial, 320 adults with non-specific cLBP were randomized receive 12 weekly yoga classes, 15 PT visits, or an educational book and newsletters in order to determine whether yoga is non-inferior to PT for cLBP. Primary outcomes were back-related function as measured by the Roland Morris Disability Questionnaire (RMDQ), and pain as measured by an 11-point scale at 12 weeks of follow-up. Researchers found that improvement in RMDQ for yoga was non-inferior to that for PT (mean difference -0.26, 1-sided 95% CI -¥ to 0.83). Yoga was also non-inferior in terms of pain reduction when compared to PT (mean difference 0.51, 1-sided 95% CI -¥ to 0.97). Limitations to this study included the fact that participants could not be blinded to treatment assignment, and disproportionate loss to follow-up in the PT group. Nonetheless, the authors of this study concluded that a manualized yoga program for non-specific cLBP was non-inferior to PT for function and pain.
With the continued aging of the population, the incidence and prevalence of dementia has increased. As there is no cure, it is important to identify modifiable risk factors and protective factors to reduce the risk of dementia. One such protective factor may be physical activity, although there is a paucity of data in this area due to limited follow-up times in studies. In this cohort study, the authors used data spanning nearly 3 decades, including 10,308 participants to investigate the association between physical activity and long-term cognitive function. Exposures included time spent in mild, moderate to vigorous, and total physical activity assessed 7 times between 1985 and 2013. Participants were considered to have met the “recommended” amount of physical activity if duration of moderate to vigorous physical activity was 2.5 hours/week or more. Researchers found no association between physical activity and risk of dementia over an average of 27 years of follow-up (HR 1.00, 95% CI 0.80 to 1.24). Similarly, no significant differences in of hours/week of total, mild and moderate to vigorous physical activity was detected in participants with dementia 10 and 28 years prior to diagnosis as compared to those without dementia. This study therefore shows that there may be no neuroprotective effect of physical activity in terms of preventing dementia.
Mammography has been shown to have a modest impact on the reduction of deaths due to breast cancer, while exposing women to a number of harms. In this study, the authors report on the results of an online survey completed by 407 women age 40 to 59 years on women’s awareness and perceptions of the benefits and harms of mammography. As part of the survey, participants were presented with 4 statements describing mammography benefits: 1) Mammograms can save lives, 2) Mammograms can lead to earlier treatment of breast cancer, 3) Mammograms can provide peace of mind by finding that you do not have breast cancer, and 4) Mammograms can find cancer early, sometimes before cancer symptoms begin. Researchers found that over 90% of participants were aware of the 4 statements describing mammography benefits, with 54.8% concluding that each benefit was “very important”. Awareness of the harms of mammography, however, was more variable, where only 26.5% of women reported prior awareness of overdiagnosis, and 39.7% of overtreatment. Conversely, 74.9% of participants were aware of false-positive results and the potential harms of psychological distress. In contrast to their evaluation of benefits, fewer women rates the harms of mammography as “very important”. Women who had a mammogram within the past year were more likely to rate all 4 benefits as “very important” (p<0.05) and less likely to rate health care system costs and radiation-related harms as “very important” (p<0.05) compared to those who had never had a mammogram. This study therefore shows that women are more aware of the benefits of mammography compared to the harms, with women having recently undergone screening being more likely to judge these benefits as important. This has important implications for the role of the physician in educating patients on the harms of mammography in addition to its benefits.
Image: PD
©2017 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
