



{kind=link}


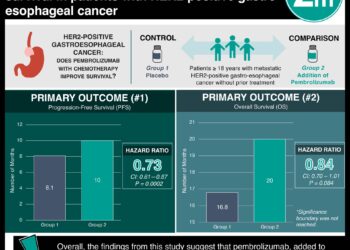
Neoadjuvant chemoradiotherapy plus surgery increases overall survival of patients with advanced esophageal squamous cell carcinoma compared to surgery alone
1. Neoadjuvant chemoradiotherapy (NCRT) with surgery improves the death rate, overall survival, disease-free survival time, and locoregional and distal recurrence rates of advanced esophageal squamous cell carcinoma compared to surgery alone
2. While NCRT incurred more adverse events, there was not more treatment-associated deaths, thus the survival benefit could potentially outweigh these risks
Evidence Rating Level: 1 (Excellent)
Study Rundown: Esophageal squamous cell carcinoma (ESCC) makes up 90% of East Asian esophageal cancer, which in turn is half of esophageal cancer. Surgery is currently the standard of care for the treatment of locally-advanced esophageal cancer, with 5-year survival rate of 25%. The Neoadjuvant Chemoradiotherapy for Esophageal Cancer 5010 randomized controlled trial previously showed benefit of neoadjuvant chemoradiotherapy (NCRT) to overall and disease-free survival at 24-months. This study, the NEOCRTEC50 trial, investigated the efficacy of NCRT with surgery on overall survival of ESCC versus surgery alone, with a primary endpoint of overall survival and secondary outcome of disease-free survival. Adults with advanced ESCC were randomized to NCRT plus surgery or surgery alone. While adverse events to NCRT were common, most completed treatment. The number of patient-related deaths did not significantly differ between treatment groups. NCRT had improved death rate, overall survival, and overall percent of participants surviving at 5-years compared to surgery alone. While most surgeries had negative margins at the time of resection, more cancer relapse and locoregional and/or distant recurrence occurred with surgery alone, shortening disease-free survival time compared to patients who also received NCRT. Strengths of this study include the size, power, and long duration of follow-up, focus on the population primarily afflicted by ESCC, and intention-to-treat analysis making conservative estimates. One drawback of this design is the burdensome treatment requiring significant exclusion criteria caused most patients to be quite young and fit, especially for a cancer study, which limits the generalizability of this data. Additionally, this data might not be applicable to a Western setting as it occurred in China where ESCC is more common.
Click to read the study in JAMA Surgery
Click to read an accompanying editorial in JAMA Surgery
Relevant Reading: A meta-analysis on surgery with or without postoperative radiotherapy to treat squamous cell esophageal carcinoma
In-Depth [randomized controlled trial]: Adults (age 18-70) with stage T1-4N1M0/T4N0M0, surgically resectable, histologically proven ESCC, who were surgical candidates with a Karnofsky score of at least 90 and had no history of other cancers or gastrectomy, were eligible for this study. Patients were computer-randomized to NCRT plus surgery or surgery alone, stratified by participating center. Age, percent male, and disease stage were balanced between groups. The NCRT group radiotherapy and chemotherapy started on the same day. Chemotherapy involved either 75 mg/m2 of cisplatin on day 1 plus 25 mg/m2 of vinorelbine on days 1 and 8 or 25 mg/m2 of cisplatin on days 1 – 4 and 22- 25. Most participants (n = 451) had T3 tumors (60.3%) and N1 nodes (86.5%), and were male (81.4%), with a mean age of 56.5±7.0 years. ESCC patients were evenly randomized, stratified by the 8 Chinese centers, into a NCRT group (n = 224; age = 56.0±7.1 years; 84.8% male; 83.9% stage III disease) and a surgery group (n = 227; age = 56.9±6.9 years; 78.0% male; 83.7% stage III disease). Adverse events were common to the NCRT group, including Grade 3 or 4 hematologic (54.3%), Grade 3 or 4 non-hematologic (7.2%), leukopenia (48.9%), and neutropenia (45.7%). 182 NCRT patients of the 185 that went on to have surgery had negative margins (98.4%). 207 of 227 surgery only patients went on to have negative margins (91.2%), fewer than NCRT (P = 0.002). Peri-treatment mortality did not significantly differ (P = 0.21) between NCRT (n = 4; 2.2%) and surgery (n = 1; 0.4%). The NCRT group had a death rate of 44.6%, while the surgery only group had one of 54.6%, thus overall survival post-operatively was higher with NCRT (HR = 0.74; 95% CI = 0.57-0.97; P = 0.03). Overall survival at 5 years with NCRT (59.9%, 95% CI = 52.9%-66.1%) compared to surgery alone (49.1%, 95% CI = 42.3%-55.6%) was higher (HR = 0.73, 95% CI = 0.55-0.97; P = 0.03), with a number needed to treat of 9.3 (95% CI = 5.0-73.2). Fewer NCRT patients experienced cancer relapse (42.3%) compared to surgery group (59.4%). Compared to surgery alone, NCRT decreased locoregional recurrence (21.7% vs 13.7%) and distal recurrence (35.7% vs 25.3%), and combined locoregional and distal recurrence of cancer (8.2% vs 4.4%). NCRT patients had longer disease-free survival times than the surgery patients (HR = 0.60; 95%CI = 0.45-0.80; P < 0.001). Similarly, a greater proportion of NCRT patients were disease-free at 5 years (63.6%, 95% CI = 56.0%-70.2%) compared with the surgery group (43.0%, 95% CI = 36.0%-49.7%) (HR = 0.55, 95%CI = 0.40-0.74; P < 0.001), with a number needed to treat of 4.9 (95% CI = 3.3-9.4). These results stand for all demographic subgroups benefiting from NCRT.
Image: PD
©2021 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
