




{kind=link}


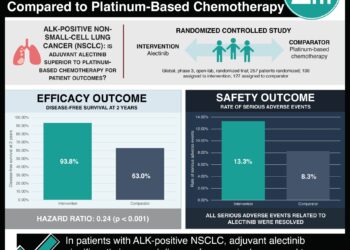
New device for continuous renal replacement therapy in small infants
Image: PD
1. Design of a machine utilizing small priming volumes and very low ultrafiltration flows makes renal replacement therapy in infants and neonates a possibility.
Evidence Rating Level: 3 (Average)
Study Rundown: Acute kidney injury is a common disorder in the adult population. However, due to historical reports that acute kidney injury occurs around 1-2% of hospitalized neonates, there has not been a large focus on treating the condition in this population until recently. Devices that currently exist are insufficient for use in infants and neonates – the large circuits in these machines require high priming volumes that can lead to hypotension in patients with total blood volumes between 200-800 mL. The authors of the current study designed and tested, through both in vitro and in vivo means, a device specifically designed for renal replacement therapy in infants weighing less than 10 kg. After production and extensive in vitro testing this device was used on one patient suffering from hemorrhagic shock, acidosis, hyponatremia, oliguria, and 63% fluid overload with successful results. This report is seminal in the design and use of a novel device specifically for renal replacement therapy in infants. A drawback to this study is that it only involved a single patient without comparison to any control treatment. Further testing is required to ensure that there are not unforeseen complications that were not revealed initially.
The study was funded by Associazione Amici del Rene di Vicenza.
Click to read the study, published today in The Lancet
Relevant Reading: Acute kidney injury in critically ill newborns: What do we know? What do we need to learn?
In-Depth [case report]: This study detailed the 5 year plan to design and utilize a device which came to be known as CARPEDIEM (Cardio-Renal Pediatric Dialysis Emergency Machine) capable of continuous renal replacement therapy in infants weighing between 2.5 and 10 kg. The authors created a machine utilizing miniaturized roller pumps and smaller dialysis circuits capable of running with continuous flows as low as 5-50 ml/min with error of less than 10%. In vitro testing showed an accuracy of ultrafiltration up to 1 g/h. Reinfusion or dialysis flow errors ranged from -8.0% to 7.5%. The observed microhemolysis index was lower than 0.7 g of plasma free hemoglobin released per 100 L of blood pumped.
The CARPEDIEM was then utilized in one patient 72 hours after birth. The patient was suffering from hemorrhagic shock, having presented with subgaleal hemorrhage caused by vacuum extraction. After 25 days and more than 400 hours on the CARPEDIEM the patient was hemodynamically stable and continuous renal replacement therapy was discontinued. The patient was successfully discharged from the hospital 59 days later with renal impairment that did not require replacement therapy.
More from this author: Link between early life antibiotic use, asthma exacerbations, and impaired viral immunity,Structural and neurobiological foundations of suicide, a review,Buccal administration of dextrose gel effective in treatment of neonatal hypoglycemia, Racial backgrounds key to shaping the face of smoking-related mortality in South Africa,Probiotic formulations do not prevent antibiotic-associated diarrhea,
©2012-2014 2minutemedicine.com. All rights reserved. No works may be reproduced without expressed written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors, editors, staff or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT.
RelatedReports
