[NEJM] Tight glycemic control versus standard care after pediatric cardiac surgery
Image: Public Domain. Pediatric surgery in Haiti.
Primer: Tight glycemic control has been shown to reduce morbidity and mortality in certain critically ill adult patients, while limited evidence is available for the pediatric population. Several studies have previously demonstrated high incidence of hyperglycemia in infants and young children after cardiac surgery, though the evidence is mixed regarding whether hyperglycemia is associated with increased perioperative morbidity. While tight glycemic control has shown some benefit, it was also linked to high rates of severe hypoglycemia (i.e., <40 mg/dL or 2.2 mmol/L), which may have harmful effects on the developing brain.
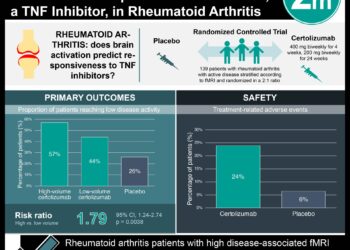
This [randomized] study: Published in The New England Journal of Medicine, a two-centre, prospective, randomized trial sought to explore whether tight hypoglycemic control in cardiac intensive care units (ICUs) would reduce perioperative morbidity in young children who had undergone cardiac surgery with cardiopulmonary bypass. The analysis included 980 patients, with half randomized to standard care and the other half randomized to tight glycemic control, which involved intravenous infusion of regular human insulin at the lowest dose required to achieve normoglycemia and continuous subcutaneous glucose monitoring with periodic blood glucose checks. The rate of severe hypoglycemia was 3% in the glycemic-control group and 1% in the standard-care group (P=0.03), while the total rate of hypoglycemia was 19% and 9%, respectively (P<0.001). All episodes of hypoglycemia were asymptomatic. Rates of hypokalemia were similar in the two groups, with 3% in the glycemic-control group and 4% in the standard-care group (P=0.60). There were no significant differences between the two groups in terms of health-care associated infections, mortality, length of stay in the cardiac ICU, or other organ-specific end-points.
In sum: This study demonstrated no significant benefit of tight glycemic control in critically ill pediatric patients who had undergone cardiac surgery. While tight glycemic control was associated with higher rates of hypoglycemia, the rate of severe hypoglycemia was quite low and all episodes were asymptomatic. These findings are notably different from those of a previous randomized trial, which demonstrated reduced mortality, length of ICU stay, and rate of infection with tight glycemic control in a mixed critical care population of medical and surgical patients. The authors note that this study was limited to pediatric patients who had undergone cardiac surgery, and could not be extrapolated to other critically ill pediatric populations.
The strengths of the study include high adherence to the study protocol and blinding of the study investigators, intraoperative care teams, and adjudicators of the primary outcome to treatment-group assignments. The limitations include not blinding bedside clinicians in the cardiac ICU to treatment-group assignments (as they were responsible for monitoring blood-glucose concentrations during insulin infusions).
Click to read the study at the NEJM database
© 2012 2minutemedicine.com. All rights reserved. No works may be republished or reproduced without written consent obtained from 2minutemedicine.com.