Patient Basics: Atrial Fibrillation
Originally published by Harvard Health.
What Is It?
Atrial fibrillation is a heart rhythm disorder that causes a rapid and irregular heartbeat.
Atrial fibrillation affects the upper two chambers of the heart, the atria. All blood circulates through both atria.
The heart is a muscle. The walls of the chambers of the heart are made of muscle cells.
Normally, the muscular walls of the atria contract at the same time, pumping blood into the lower two chambers (the ventricles). Then the walls of the ventricles contract at the same time, pumping blood to the rest of the body.
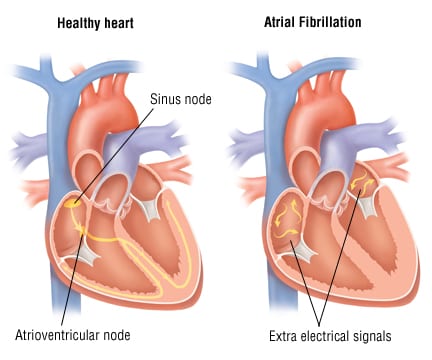
For the heart to work efficiently, the atria need to pump first, and then the ventricles need to pump. How is this coordinated? Normally, each heartbeat starts with an electrical impulse that comes from a small part of the atrium called the sinus node. That signal first causes the atria to beat, pumping blood into the ventricles. Then the signal travels to another part of the heart called the atrioventricular node. From there, the signal travels down to the ventricles, and causes them to beat, sending blood throughout the body.
In contrast, during atrial fibrillation, instead of one coordinated signal that causes all parts of the atria to pump at the same time, there are multiple uncoordinated signals. Instead of pumping efficiently, the atria just quiver.
As a result, the atria do not pump all of their blood into the ventricles. Also, the ventricles sometimes pump when they don’t have a lot of blood in them. So the heart is not pumping efficiently.
In atrial fibrillation, the heartbeat is rapid and irregular. A normal heartbeat is 60 to 100 beats per minute, and very regular: beat…beat…beat…beat. During atrial fibrillation, the heart beats at 80 to 160 beats per minute, and is very irregular: beat..beat…..beat….beat.beat.beat….beat.
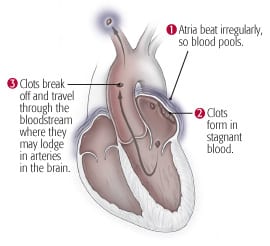
Atrial fibrillation can lead to the formation of blood clots inside the atria. That’s because blood tends to form clots when it’s not moving. The quivering atria don’t move all of the blood along to the ventricles. Some blood just pools inside the atria, and the pool of still blood tends to form clots.
Such blood clots can cause serious problems. They can travel out of the heart and get stuck in an artery to the lungs (causing a pulmonary embolism), an artery to the brain (causing a stroke) or an artery elsewhere in the body.
The major factors that increase the risk of atrial fibrillation are:
- Age
- Coronary artery disease
- Rheumatic heart disease
- High blood pressure
- Diabetes
- An excess of thyroid hormones
Symptoms
Atrial fibrillation often doesn’t cause any symptoms. When symptoms occur, they can include:
- Palpitations (awareness of a rapid heartbeat)
- Fainting
- Dizziness
- Weakness
- Shortness of breath
- Chest pain
Some people with atrial fibrillation have periods of normal heartbeats: the atrial fibrillation comes and goes. In many others, the atrial fibrillation becomes a constant condition, one that remains for the rest of their lives.
Diagnosis
Your doctor will ask about your family history of cardiovascular disorders. He or she will review your personal medical history. This includes any possible risk factors for atrial fibrillation.
Your doctor will ask about your specific heart symptoms, including possible triggers for your symptoms.
Your doctor will examine you. He or she will check your heart rate and rhythm and your pulse. In atrial fibrillation, your pulse often doesn’t match your heart sounds.
The diagnosis of atrial fibrillation is usually confirmed with an electrocardiogram (EKG). An EKG is a test that records the heart’s electrical activity. However, because atrial fibrillation can come and go, a standard EKG may be normal.
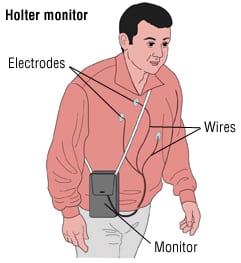
If this is the case, an ambulatory EKG may be done. During this test, the patient wears a portable EKG machine (Holter monitor). The Holter monitor is usually worn for 24 hours.
If your symptoms appear less frequently than once a day, your doctor may use an event recorder. You keep an event recorder with you for several days or even weeks. It attempts to capture your heart rhythm at the time you feel an irregular beat.
Expected Duration
How long the condition lasts depends on the cause. Atrial fibrillation caused by a treatable condition may go away when the condition is treated.
However, atrial fibrillation is often a lifelong condition. This is more likely when it has no known cause or results from a long-standing cardiac disorder.
Prevention
Atrial fibrillation resulting from coronary artery disease can be prevented. Take these actions to reduce your risk:
- Eat a low-fat diet.
- Control cholesterol and high blood pressure.
- Do not drink more than two alcoholic drinks per day.
- Quit smoking.
- Control your weight.
- Get regular exercise.
Some causes of atrial fibrillation cannot be prevented.
Treatment
Treating the Likely Causes
Treatment depends on the cause.
If the cause is coronary artery disease, treatment may consist of:
- Lifestyle changes
- Cholesterol-lowering medications
- Blood pressure medications
- Angioplasty
- Coronary artery bypass surgery
Atrial fibrillation caused by an excess of thyroid hormones can be treated with medication or surgery. When rheumatic heart disease is the cause, the condition may be treated with surgery to replace heart valves damaged by the disease.
Treatment of the First Attack
When a person develops atrial fibrillation for the first time (or the first few times), doctors often try to restore a normal heart rhythm. This is particularly true if a person is having bothersome symptoms (like shortness of breath or weakness) from atrial fibrillation. Even if the person is not having symptoms, there is a reason to try to restore a normal rhythm: the longer the heart is left to remain in atrial fibrillation, the harder it is to restore a normal heart rhythm.
Several different medicines are used to restore a normal heart rhythm. Another treatment option is electrical cardioversion: a small shock is delivered to the chest, and the electricity can “re-set” the heart to a normal rhythm. This procedure works in most cases. But more than half of patients eventually develop atrial fibrillation again.
Another treatment to try to keep the heart from repeatedly going back into atrial fibrillation is radiofrequency catheter ablation. This procedure is typically performed in a catheterization laboratory of a hospital. The procedure uses radio waves to destroy tissue in the heart that is triggering the abnormal electrical rhythms that cause atrial fibrillation. If it is effective in eliminating recurrent attacks of atrial fibrillation, then it also eliminates the symptoms caused by atrial fibrillation as well as the risk of blood clots and the risks of the blood thinners needed to prevent blood clots.
Unfortunately, radiofrequency catheter ablation is not always effective, and also can produce serious adverse effects. So you need to talk to the doctor about the balance of benefits and risks.
Another surgical procedure involves creating scars in the atria. This hinders abnormal electrical activity from spreading and causing atrial fibrillation.
Keeping A Normal Heart Rhythm
When a normal heart rhythm has been restored, several different medicines may be given to try to hold the heart in a normal rhythm. This is called “rhythm control”.
Sometimes, high doses of beta-blocker drugs can hold the heart in a normal rhythm. These drugs have relatively few serious adverse effects. For most patients, however, the most potent drugs for keeping the heart out of atrial fibrillation are the antiarrhythmic drugs, such as amiodarone, flecainide, dofetilide, propafenone, and sotalol. Although these drugs are more potent, they also can have serious side effects.
Slowing the Heart Rate
Sometimes—usually after the heart has slipped back into atrial fibrillation several times, despite treatment—doctors decide it is better to leave the heart in atrial fibrillation. When that happens, the heart rate usually needs to be slowed down to help the heart work most efficiently. This is called “rate control”.
Medicines used to slow the heart rate include beta blockers, calcium-channel blockers, and digoxin.
Rhythm Control Versus Rate Control
For the average person with atrial fibrillation, large studies have found that rhythm control and rate control have approximately the same long-term consequences: one is not superior to the other.
Anticoagulation
For anyone who has chronic atrial fibrillation, or who may be going in and out of atrial fibrillation without knowing it (because it doesn’t cause them symptoms, the risk of blood clots needs to be reduced. This requires “blood thinning” drugs.
The drug used most often is warfarin. This drug has been used in millions of patients over more than 70 years. Doctors have lots of experience in using it, and lots of knowledge about its possible side effects. Like any blood thinning drug, it has risks: a drug that reduces the risk of blood clotting thereby increases the risk of bleeding. Warfarin also needs to be monitored regularly: you need periodic blood tests to make sure the dose of warfarin has thinned the blood just enough and not too much.
There are several newer drugs that have become available or may soon be available, that do not require the periodic monitoring of warfarin, and that may have a lower risk of bleeding. They are considerably more expensive, and because they are new there is less known about their possible side effects than warfarin.
For some people, the best blood thinning drug is aspirin.
When To Call a Professional
Call your doctor if you have any of the symptoms of atrial fibrillation. This includes:
- Palpitations
- Faintness
- Dizziness
- Weakness
- Shortness of breath
- Chest pain
Prognosis
When a cause of atrial fibrillation is identified and treated, the arrhythmia often goes away. It is less likely to go away in people who have long-standing rheumatic heart disease or any condition in which the atria are enlarged.
Blood thinning medications can reduce the risk of a stroke or other complications.
Additional Info
American Heart Association (AHA)
7272 Greenville Ave.
Dallas, TX 75231
Toll-Free: 1-800-242-8721
http://www.americanheart.org/
National Heart, Lung, and Blood Institute (NHLBI)
P.O. Box 30105
Bethesda, MD 20824-0105
Phone: 301-592-8573
TTY: 240-629-3255
Fax: 301-592-8563
http://www.nhlbi.nih.gov/
American College of Cardiology
Heart House
9111 Old Georgetown Road
Bethesda, MD 20814-1699
Phone: 301-897-5400
Toll-Free: 1-800-253-4636, ext. 694
Fax: -301-897-9745
http://www.acc.org/
RelatedReports