No products in the cart.

Patient Basics: Hysterectomy
Originally published by Harvard Health.
What Is It?
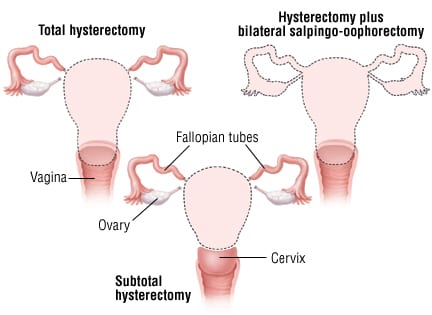
A hysterectomy is the surgical removal of the uterus. Depending on the type of hysterectomy, other pelvic organs or tissues also may be removed. The types of hysterectomy include:
- Subtotal, supracervical or partial hysterectomy. The uterus is removed, but not the cervix.
- Total or complete hysterectomy. Both the uterus and the cervix are removed.
- Total hysterectomy plus unilateral salpingo-oophorectomy. This procedure removes the uterus, cervix, one ovary and one fallopian tube, while one ovary and one fallopian tube are left in place. This procedure is usually done if a problem confined to one ovary is detected at the time of hysterectomy. After surgery, the remaining ovary should produce enough female hormones if the woman has not reached menopause.
- Total hysterectomy plus bilateral salpingo-oophorectomy. This is the removal of the uterus, cervix, and both fallopian tubes and ovaries. Removing both ovaries will cause surgical menopause in a woman who has not reached menopause because the production of female hormone stops when the ovaries are removed.
- Radical hysterectomy. This procedure removes the uterus, cervix, both ovaries, both fallopian tubes and nearby lymph nodes in the pelvis. This procedure is only done in some women who have gynecological cancer.
Hysterectomies can be done with different types of surgical incisions (surgical cuts). Until recently most hysterectomies were abdominal hysterectomies, in which the uterus is removed through a horizontal or vertical incision in the lower abdomen.
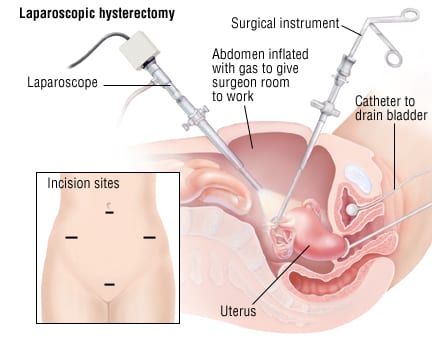
Now about 50% of hysterectomies are done using a laparoscope, a telescope-like instrument with a camera for viewing inside the abdomen. The surgeon makes several small incisions in the abdomen that allow the insertion of instruments to help remove the uterine attachments. Once freed from its attachments, the uterus can be removed either through the vagina (laparoscopic assisted vaginal hysterectomy) or in pieces through the small abdominal incisions (total laparoscopic hysterectomy). As laparoscopic techniques continue to improve, the number of hysterectomies done by this approach will increase.
Vaginal hysterectomies, in which the uterus is removed through an incision in the vagina, are done about 20% of the time. When considered equally safe, most experts prefer the vaginal approach rather than a traditional abdominal hysterectomy because the recovery time is much faster.
Hysterectomy is a very common surgical procedure in the United States, especially in middle-aged women between 40 and 50. About one out of every three women in the United States eventually has a hysterectomy.
What It’s Used For
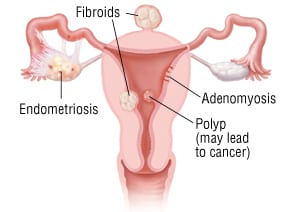
About one-third of all hysterectomies are done because the uterus is enlarged with fibroids, which are benign (noncancerous) growths of muscle fibers in the uterus. About one of 10 hysterectomies are done to treat uterine cancer, and about one of 20 of the surgeries are done because of severe menstrual bleeding problems. Hysterectomies also are used to treat a prolapsed uterus, endometrial hyperplasia (abnormal growth of the uterine lining which may lead to cancer) or endometriosis.
Uterine polyps are almost always benign. In rare instances, hysterectomy might be the best option for removal.
Preparation
Because a hysterectomy removes the uterus, this surgery will prevent you from ever becoming pregnant. If you wish to remain fertile, you should ask your doctor if there is any other treatment for your gynecological problem. If there is any chance that you might be pregnant, you should be tested carefully by your doctor before surgery.
You may have preliminary blood tests, a urinalysis, an electrocardiogram (EKG) and a chest X-ray to make sure there are no undiagnosed medical problems that could complicate your surgery. A pelvic ultrasound may be done to evaluate the uterus and ovaries, depending on your medical history and physical exam. Beginning at least eight hours before surgery, you must not eat or drink anything. This reduces the risk of vomiting during surgery. Most women are asked not to eat or drink anything after midnight before surgery to allow the stomach to be as empty as possible. Antacids commonly are given just before surgery to counteract any remaining stomach acids and to further reduce the risk of vomiting.
How It’s Done
A hysterectomy takes about one to two hours. You will either be under general anesthesia or have regional anesthesia during the surgery. Regional anesthesia is by spinal or epidural injection of medicines to numb the lower half of your body. Before the procedure, an intravenous (IV) catheter will be inserted into one of your veins to deliver fluids and medications. What happens next depends on the type of hysterectomy:
- Abdominal hysterectomy. The surgeon will make a 5-inch to 7-inch incision in your lower abdomen. The incision can be vertical (from the belly button to just above the pubic bone) or transverse (horizontal at the pubic-hair line, often called a “bikini incision”). The uterus is freed from its attachments to blood vessels and supportive tissues, and then is removed through the incision. Then the layers of the abdomen will be closed with sutures (stitches) and the incision may be closed with sutures or titanium (metal) staples. Staples or non-dissolving skin sutures usually are removed about one week after the surgery.
- Vaginal hysterectomy. An incision will be made in the wall of the upper portion of your vagina. Through this incision, the surgeon will use sterile instruments to detach your uterus and to tie off nearby blood vessels. Your uterus will be removed through your vagina, and then the incision will be stitched closed. Once the vagina has healed, the length of the vagina should remain adequate for comfortable sexual intercourse.
- Laparoscopic hysterectomy. Three or four small incisions are made in the wall of the abdomen to allow the surgeon to insert a laparoscope and additional surgical instruments. In some cases a robot is used to control the instruments. These instruments are used to help free the main body of the uterus and to remove the ovaries, if necessary. The uterus is then removed either through the vagina or through the small abdominal incisions. At the end of the procedure, the upper portion of the vagina is stitched closed and the small abdominal incisions are closed with sutures or surgical tape.
After your surgery, you will be taken to a recovery room. There, your vital signs (blood pressure, heart rate, breathing rate and temperature) will be monitored closely, and you will be given pain medication if needed. After a few hours, you will be taken to your hospital room to rest and to begin healing. Your IV line will be removed, and you will be allowed to eat as soon as your digestive system is ready to handle liquids and solid food. You may remain in the hospital for one to three days. During the first few days after your hysterectomy, you may have slight vaginal bleeding and discharge.
Follow-Up
Before you leave the hospital, your doctor will tell you when to schedule a follow-up office visit. At this visit, your doctor will check the healing of your incisions and remove any sutures or staples. If you have had an abdominal hysterectomy, the soreness at your incision site should ease gradually over a period of about two to three weeks and the strength of the incision heals in about six weeks. In most cases, you can resume sexual intercourse in six weeks. Talk with your doctor for guidance about resuming sexual intercourse and other activities (exercising, driving, sports, lifting).
Risks
While not common, possible complications from a hysterectomy include but are not limited to:
- Excessive bleeding
- Infection
- An injury to the bowel or bladder
- An injury to nerves that regulate the bladder, causing either incontinence or overfilling of the bladder
- A blood clot in the veins of the legs (called deep venous thrombosis). If such a clot floats out of the leg and lodges in the lungs, it is a more dangerous complication called a pulmonary embolism.
When To Call a Professional
Once you return home, call your doctor immediately if you develop any of the following problems:
- Fever
- Excessive bleeding from your vagina
- Bleeding, discharge, swelling or extreme tenderness at your incision site
- Nausea, vomiting or abdominal pain
- Trouble urinating
- Feelings of excessive sadness
- Difficulties or discomfort during sexual intercourse (once the gynecologist says it’s OK to resume sex)
Additional Info
American College of Obstetricians and Gynecologists
P.O. Box 96920
Washington, DC 20090-6920
Phone: 202-638-5577
http://www.acog.org/
RelatedReports



