



{kind=link}


Quick Take: Randomized Trial of Intravenous Versus Intraperitoneal Chemotherapy Plus Bevacizumab in Advanced Ovarian Carcinoma
Recent advances have been demonstrated with the administration of intraperitoneal (IP) cisplatin and paclitaxel, where women with stage III ovarian disease conferred additional survival benefit as compared to conventional intravenous (IV) chemotherapy. However, due to concerns surrounding toxicity and difficulty administering IP therapy, less than half of the eligible women treated at National Cancer Institute (NCI) comprehensive cancer centers have received it. This points to a need for a less complicated, less toxic, and more feasible outpatient regimen to increase access. In this randomized controlled trial, 1560 patients with newly diagnosed advanced ovarian carcinoma were randomly assigned to receive IV carboplatin, IP carboplatin, or IP cisplatin to evaluate the impact of two different IP chemotherapy regimens on progression-free survival (PFS). The specific treatment regimens consisted of the following: 1) 6 cycles of IV paclitaxel 80 mg/m2 once weekly with IV carboplatin, 2) IV paclitaxel 80 mg/m2 once weekly with IP carboplatin, or 3) once every 3 weeks IV paclitaxel 135 mg/m2 over 3 hours day 1, IP cisplatin 75 mg/m2 day 2, and IP paclitaxel 60 mg/m2 day 8. All participants received bevacizumab 15 mg/kg IV every 3 weeks in cycles 2 to 22. Researchers found that the median PFS duration was 24.9 months in the IV carboplatin arm, 27.4 months in the IP carboplatin arm, and 26.2 months in the IP cisplatin arm. For the subgroup of 1,380 patients with stage II/III and residual disease of 1 cm or less, median PFS was 26.9 months (IV-carboplatin), 28.7 months (IP-carboplatin), and 27.8 months (IP cisplatin), respectively. Compared to IV carboplatin, time to first progression or death was 7.5% lower in the IP carboplatin arm (HR 0.925, 95% CI 0.802 to 1.07) and 2.3% lower in the IP cisplatin arm (HR 0.977, 95% CI 0.847 to 1.13); neither of these differences were statistically significant. The median PFS for patients with stage II/III and no residual disease was 35.9 months for carboplatin, 38.8 months for IP carboplatin, and 35.5 months for IP cisplatin; again there were no statistically significant differences in this subgroup of patients. The median overall survival for all enrolled was 75.5, 78.9, and 72.9 months, respectively. The mean patient-reported Functional Assessment of Cancer Therapy neurotoxicity scores were similar for all treatment arms, however, the mean Trial Outcome Index of the Functional Assessment of Cancer Therapy-Ovary scores during chemotherapy were statistically worse in the IP cisplatin arm. In terms of safety, grade 3 of worse infections were more frequent in the IP arms (p=0.008), as was the incidence of nausea and vomiting, particularly in the IP cisplatin group at 11.0%. Grade 3 or worse hypertension was also significantly worse in the IP cisplatin arm (p<0.005) as compared to the IV carboplatin reference group. This study therefore shows that compared to IV carboplatin, PFS is not statistically increased with either IP carboplatin or IP cisplatin when combined with bevacizumab, putting into question the role of IP administration of chemotherapy in this patient population.
Click to read the study in Journal of Clinical Oncology
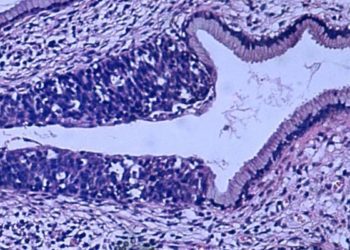
Image: PD
©2019 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
