No products in the cart.

#VisualAbstract: Low-molecular-weight heparin does not improve live birth rates in women with recurrent pregnancy loss and thrombophilia
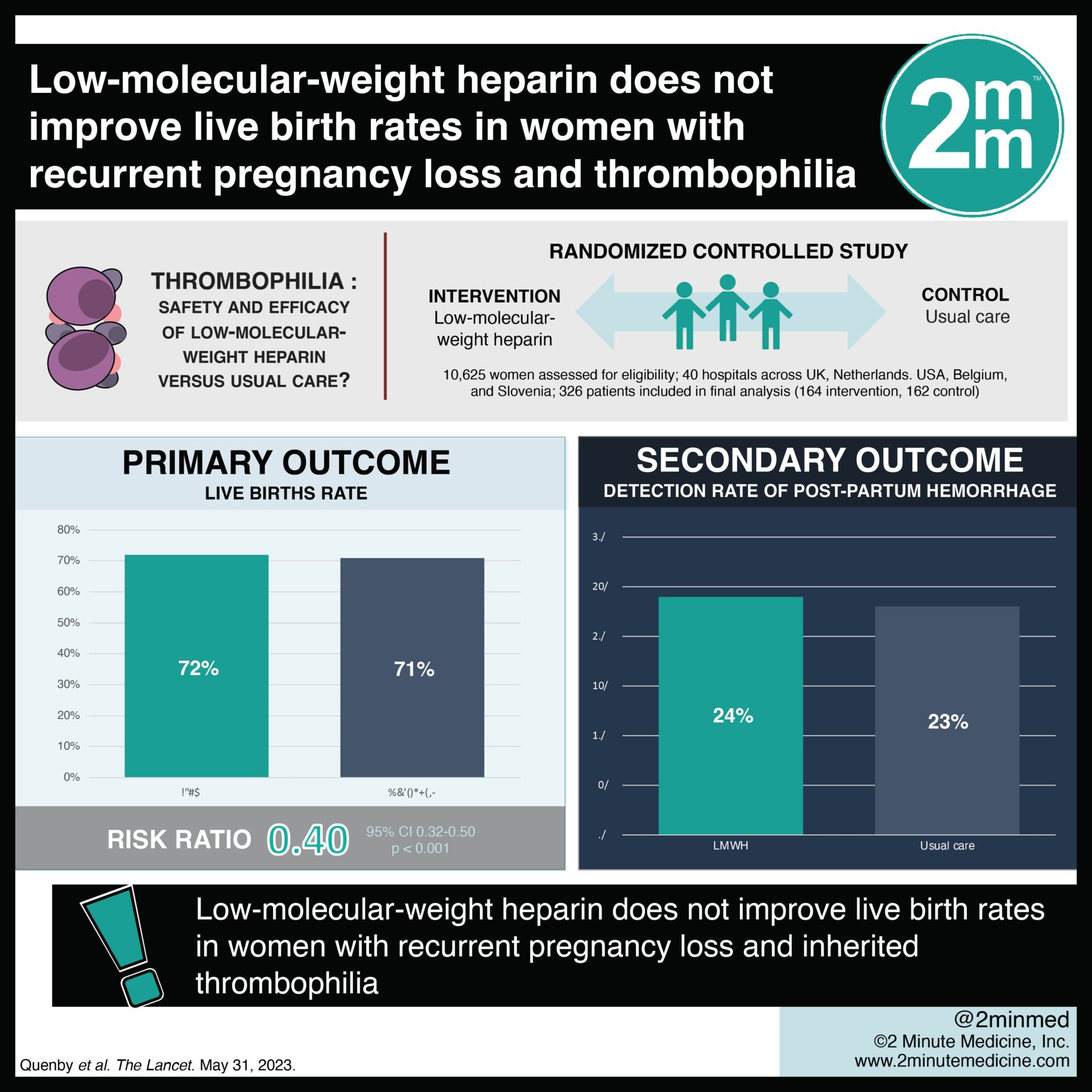
1. Live birth rate between the low-molecular-weight heparin and standard care group was comparable.
2. The most common inherited thrombophilia were heterozygous Factor V Leiden followed by heterozygous Prothrombin G20210A mutations.
Evidence Rating Level: 1 (Excellent)
Study Rundown: Thrombophilia is a leading cause of recurrent miscarriage around the world. Although anticoagulant therapy may reduce the number of miscarriages and adverse pregnancy outcomes, the recommendation for low molecular weight heparin (LMWH) has been most studied in patients with antiphospholipid syndrome. In patients with inherited thrombophilia such as Factor V Leiden mutation, prothrombin G20210A mutation, and protein C and S deficiencies, there is limited evidence supporting the use of heparin. This randomized controlled trial aimed to investigate the effectiveness of LMWH compared to standard care in reducing miscarriages and adverse pregnancy outcomes in women with recurrent pregnancy loss and inherited thrombophilia. The primary outcome of this study was the livebirth rate, while a key secondary outcome was the assessment of safety outcomes such as bleeding episodes, thrombocytopenia, and skin reactions. According to study results, there were no differences in live birth rates between the LMWH and standard care groups. Although this study was well done, it was limited by a relatively small sample size.
In-depth [randomized-controlled trial]: Between Aug 1, 2012, and Jan 30, 2021, 10 625 women were assessed for eligibility across 40 hospitals in the UK, Netherlands, USA, Belgium, and Slovenia. Included were patients aged 18–42 years with ≥ 2 pregnancy losses and confirmed inherited thrombophilia, who were trying to conceive or were ≤ 7 weeks pregnant. Altogether, 326 patients (164 in LMWH and 162 in standard care) were included in the final analysis. The most common inherited thrombophilia in this cohort were heterozygous Factor V Leiden mutation (58% and 55%), heterozygous Prothrombin 20210A mutation (24% and 27%), and Protein S deficiency (14% and 13%) in the LMHW and standard care groups, respectively. There was no significant difference in the primary outcome of live birth rate between both groups (72% in the LMWH group vs. 71% in the standard care group, odds ratio [OR] 1.08, 95% confidence interval [CI] 0.65-1.78, absolute risk difference 0.7%). This was also the case for the secondary outcome concerning adverse events (24% in LMWH vs. 23% in standard care). Findings from this study suggest that LMWH does not improve live birth rates in women with recurrent pregnancy loss and inherited thrombophilia.
©2023 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports

{kind=link}
