
Catheter ablation more effective than antiarrythmic escalation for ventricular tachycardia: The VANISH trial
1. Catheter ablation was found to be more effective than escalated antiarrhythmic drug (AAD) therapy at treating patients with ischemic cardiomyopathy and an implantable cardioverter-defibrillator (ICD) who had ventricular tachycardia (VT) despite AAD therapy.
2. The increased effectiveness was only observed in patients treated with amiodarone at baseline.
Evidence Rating Level: 1 (Excellent)
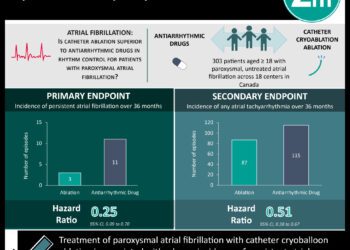
Study Rundown: Despite the effectiveness of ICDs at stopping VT secondary to myocardial infarction (MI), recurrent shocks carry health risks and these patients often require AAD therapy to suppress inducible ventricular tissue. When both fail to suppress VT, escalation of AAD therapy or catheter ablation is used. This study compared the efficacy of these two treatment options. The results demonstrated that the primary outcome of death at any time, refractory VT (defined as three or more episodes within 24 hours), or appropriate ICD shock within 30 days of treatment was significantly lower in the catheter ablation group as compared with the AAD escalation group. The significance of the primary outcome was largely due to a reduction in refractory VT and appropriate ICD shocks. However, this difference was only observed in patients receiving amiodarone at baseline. No difference was found using other AAD medications.
This study was randomized and conducted at tertiary centers where catheter ablation was routinely performed. All outcome measures and treatments used current clinical standards. Due to the type of therapy, however, the treating physicians could not be fully blinded to treatment arms.
Click to read the study, published today in NEJM
Relevant Reading: Prophylactic catheter ablation for the prevention of defibrillator therapy
In-Depth [randomized controlled trial]: This randomized controlled trial enrolled 259 patients (132 assigned to undergo catheter ablation and 127 to escalated AAD therapy) with a previous MI, subsequent placement of an ICD, and had experienced VT within 6 months of treatment with a class I or III AAD. Other outcomes included the factors contributing to the primary outcome. Patients in the escalated-therapy group were treated with amiodarone +/- mexiletine.
The overall primary outcome, was significantly reduced in the ablation group compared to escalation of AAD therapy (HR 0.72; 95%CI 0.53 to 0.98; p = 0.04). However, this difference was only observed in patients treated with amiodarone at baseline (HR 0.55, 95%CI 0.38 to 0.80; p = 0.001) but not in patients treated with other AADs (p = 0.64). Additionally, there was no significant difference in individual components of the primary outcome: death during the trial (HR 0.96; 95%CI 0.60 to 1.53; p = 0.86), VT storm (HR 0.66; 95%CI 0.42 to 1.05; p = 0.08), and appropriate ICD shocks (HR 0.77; 95%CI 0.53 to 1.14; p = 0.19). Sustained VT below ICD detection at any time (HR 0.27; 95%CI 0.09 to 0.84; p = 0.02) and total number of these events (p = 0.02) were significantly reduced in the ablation group. Among adverse events, hepatic dysfunction (6 vs. 0 patients, p = 0.001), tremor or ataxia (6 vs. 0 patients, p = 0.01), and drug side effects (6 vs. 0 patients, p = 0.01) were significantly more common in the escalation therapy group.
Image: PD
©2016 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports




{kind=link}
