
2 Minute Medicine Rewind March 21, 2016
Safety of Seasonal Influenza Vaccination in Hospitalized Surgical Patients: A Cohort Study
There are concerns about the potential side effects of influenza vaccinations that develop in the perioperative period, specifically the development of vaccine-associated fever or myalgia. It is thought that these symptoms may be incorrectly attributed to an infectious complication of the surgery and necessitate unnecessary work up. In this retrospective cohort study, 42,777 patients from the KPSC health care system in California were evaluated to determine whether influenza vaccination in the perioperative period increased health utilization. The primary outcomes included rates of outpatient visits, readmission, or ED visits in the 7 days after discharge. Resulted showed that the vaccine was administered in 6,420 of 42,777 patients. There were no differences between the vaccinated and unvaccinated groups in regards to inpatient visits (RR 1.12, 95% CI: 0.96 to 1.32), ED visits (RR 1.07, CI: 0.96 to 1.20), post discharge fever (RR 1.00, CI, 0.76 to 1.31), or clinical evaluations for infection (RR 1.06, CI, 0.99 to 1.13). However, the risk for outpatient visits was marginally elevated (RR 1.05, CI: 1.00 to 1.10; P = 0.032). The main limitation of this study was that it did not distinguish between planned and unplanned readmissions. In conclusion, this study showed that administration of the influenza vaccination during the perioperative period did not increase health care utilization subsequent to discharge.
Reintubation Among Patients With Hypoxemic Respiratory Failure Following Abdominal Surgery
Acute respiratory failure is a major contributor to the mortality and morbidity associated with abdominal surgery. Noninvasive ventilation (NIV) has been shown to be effective in nonsurgical cases, particularly in COPD and cardiogenic pulmonary edema. This study was a multicenter, randomized, parallel-group clinical trial between May 2013 and September 2014 involving 293 patient’s undergone abdominal surgery and developed hypoxemic respiratory failure. The study evaluated the effect of NIV versus standard oxygen therapy in rate of tracheal intubation within 7 days of randomization. Results showed that reintubation occurred in 49 of 148 patients (33.1%) in the NIV group and in 66 of 145 patients (45.5%) in the standard oxygen therapy group (absolute difference −12.4%; 95% CI: −23.5% to −1.3%; P = .03). Furthermore, NIV was associated with more invasive ventilation–free days compared with standard oxygen therapy (25.4 versus 23.2 days; absolute difference −2.2 days; 95% CI: −0.1 to 4.6 days; P = .04). Additionally, patients on NIV developed fewer cases of health-care associated infections (31.4% versus 49.2%; absolute difference −17.8%, 95% CI: −30.2% to −5.4%; P = .003). In conclusion, this study showed that among patients with hypoxemic respiratory failure following abdominal surgery, use of NIV compared with standard oxygen therapy reduced the risk of tracheal reintubation within 7 days.
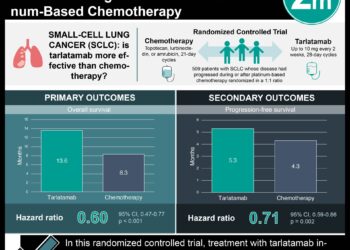
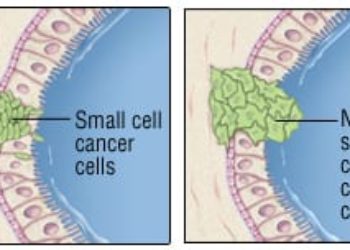
Due to the low incidence of lung cancer, screening for pulmonary nodules is an inefficient process requiring the screening of many individuals to identify intervenable early lesions. The significance of negative results on initial surveillance imaging on prognosis and morbidity is unknown. This study was a retrospective analysis of data of 26,231 patients from the NLST, a randomized, multicenter screening trial that recruited participants who were at high risk for lung cancer from 33 US medical centers. The aim of the study was to focus the rate of lung cancer incidence and mortality in patients who had a negative prevalence screen on low-dose CT and compare it to the mortality if the prevalence screen had not been done. Results showed that the 19,066 patients with a negative T0 screen had a lower rate of lung cancer incidence than did all 26,231 T0-screened participants (371.88, 95% CI: 337.97 to 408.26) per 100,000 person-years versus 661.23 (622.07-702.21). They also had a lower rate of lung cancer-related mortality (185.82, 95% CI: 162.17-211.93) per 100,000 person-years versus 277.20 (252.28-303.90). Lastly, the study suggested that if the T1 screen had not been done in the T0 negative group, 28 patients in the T0 negative group would have died from lung cancer, an increase in mortality from 185.82 (95% CI: 162.17-211.93) per 100,000 person-years to 212.14 (186.80-239.96) over the course of the trial. In conclusion, this study showed that patients with a negative-low dose CT prevalence screen had a lower incidence of lung cancer and lung cancer-related mortality than all eligible patients who underwent the prevalence screen.
Delirium is associated with increased mortality, especially in the setting of critical illness. Agitated delirium is problematic in patients receiving mechanical ventilation because it increases the risk of self-extubation. This study was a double-blind, placebo-controlled, parallel-group randomized clinical trial in Austria and New Zealand between May 2011 and December 2013 involving 74 adult patients that studied the effectiveness of dexmedetomidine on patients with agitated delirium receiving mechanical ventilation. The primary outcome was ventilator-free hours in the 7 days following randomization. Results showed that dexmedetomidine increased ventilator-free hours at 7 days compared with placebo (median 144.8 hours versus 127.5 hours, respectively; median difference 17.0 hours, 95% CI: 4.0 to 33.2 hours; P = .01). Furthermore, dexmedetomidine use was associated with reduced time to extubation (median 21.9 hours versus 44.3 hours with placebo; median difference 19.5 hours, 95% CI: 5.3 to 31.1 hours; P < .001) and accelerated resolution of delirium (median 23.3 hours versus 40.0 hours; median difference 16.0 hours, 95% CI: 3.0 to 28.0 hours; P = .01). In conclusions, among patients with agitated delirium receiving mechanical ventilation in the ICU, the addition of dexmedetomidine to standard care resulted in more ventilator-free hours at 7 days.
Gradual Versus Abrupt Smoking Cessation: A Randomized, Controlled Noninferiority Trial
Evidence conflicts as to the best approach for smoking cessation. Conventional wisdom suggests that stopping gradually leads to lower rates of relapse than abruption discontinuation. This study was a randomized, controlled noninferiority trial in England involving 697 patients with tobacco addiction that evaluated this hypothesis. Patients were randomized 1:1 to gradual or abrupt cessation. The primary outcome was prolonged validated abstinence from smoking 4 weeks after quit day. Both groups received behavioral support from clinic staff and used nicotine replacement before and after quit day. Results showed that at 4 weeks, less patients in the gradual cessation group were abstinent compared to those in the abrupt cessation group (39.2% versus 49.0%, RR 0.80, CI: 0.66 to 0.93). At 6 months, there continued to be increased abstinence in the abrupt cessation group (15.5% versus 22.0%, RR 0.71, CI: 0.46 to 0.91). Most importantly, participants who preferred gradual cessation were significantly less likely to be abstinent at 4 weeks than those in the preferred abrupt cessation group (38.3% versus 52.2%; P = 0.007). In conclusion, this study showed that quitting abruptly is more likely to lead to lasting abstinence than cutting down gradually.
Image: PD
©2016 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.



![Adverse pregnancy outcomes associated with thrombophilias [Classics Series]](https://www.2minutemedicine.com/wp-content/uploads/2015/07/Classics-2-Minute-Medicine-e1436017941513-75x75.png)

{kind=link}