
2 Minute Medicine Rewind March 23 – March 30, 2014
Image: PD
In this section, we will highlight the key high-impact studies, updates, and analyses published in medicine during the past week.
Multistate Point-Prevalence Survey of Health Care-Associated Infections
Health care-associated infections are widespread, but no universal surveillance system is in place to monitor the status of such infections on a national scale. In this retrospective analysis of randomly selected inpatient records, investigators identified the number of health care-associated infections on a single day at each of 183 hospitals (51% small, 37% medium, 12% large) across 10 geographically varied states in order to more accurately estimate the prevalence, distribution, and burden of such infections. Out of 11,282 hospitalized patients, 452 (4%) patients had at >1 health care-associated infection, and 11.5% of patients with known outcomes died during their hospitalization. Pneumonia (22%), surgical-site (22%), gastrointestinal (17%), urinary tract (13%), and primary bloodstream (10%) infections were the most common types of infection. The most common pathogens were Clostridium difficile (12%), Staphylococcus aureus (11%), Klebsiella (pneumoniae or oxytoca) (10%), and E. coli (9%). Researchers estimated that 648,000 patients developed one or more health-care associated infections in 2011. The prevalence of health care-associated infections was lower than expected based on older data.
Glycated Hemoglobin Measurement and Prediction of Cardiovascular Disease
Although some guidelines have suggested using glycated hemoglobin (HbA1c) measurements in assessing cardiovascular disease risk in non-diabetics, it is unclear what prognostic value it may add when considered with other cardiovascular risk factors (age, sex, smoking status, blood pressure, cholesterol). In this analysis of prospectively collected data from Emerging Risk Factors Collaborators, researchers examined data from 294,998 participants with no known cardiovascular disease (CVD) or diabetes at baseline to determine whether including HbA1c values in CVD risk models improved prediction of 10-year CVD risk. During a mean follow-up of 9.9 years and 20,840 cardiovascular outcomes (coronary artery disease or strokes at age >40), researchers found J-shaped associations between glycemic measures (HbA1c or fasting, random, or postload blood glucose level) and CVD risk. Adding measures of HbA1c or blood glucose improved risk discrimination of CVD outcomes marginally (by .0018 points [95% CI .0003-0.0033], from a C-index of 0.7434), and had no significant impact on 10-year risk classification (net reclassification improvement 0.42, 95%CI -0.63–1.48). Thus, although HbA1c is correlated with 10-year CVD risk in individuals without CVD or diabetes at baseline, when added to traditional risk models of CVD, it did not improve 10-year risk classification.
The Affordable Care Act’s Medicaid expansion to include anyone with an income below 133% (+5% buffer) of the federal poverty level is being adopted in 25 states and Washington, D.C., in 2014, and is expected to provide coverage to millions of adults. It is important know how this influx will change the overall population receiving Medicaid benefits, as many will be healthy but others will have chronic conditions requiring care. In this retrospective analysis of pooled 2005-2010 Medical Expenditure Panel Survey data, investigators compared non-disabled Medicaid enrollees (6.8 million), those who were eligible pre-expansion but not enrolled (4.3 million), and those who are newly eligible (23.3 million), in order to predict demographic characteristics and health status of those who are expected to be newly enrolled. Compared to pre-ACA enrollees, those who were newly eligible were found to be concentrated in the South, male, non-Hispanic white, slightly older, single, more educated, and comfortable speaking English (p<.001 for all). Newly eligible individuals reported similar overall physical and mental health status compared to existing enrollees, and were less likely to have asthma (5.6% vs 7.8%), diabetes (5.9% vs 7.7%), or be obese (28.4% vs 35.3%, p<.01 for all). While 60% of those who are newly eligible were uninsured and may underreport illnesses, obesity was calculated from self-reported height and weight, which are unlikely to affected by insurance status.
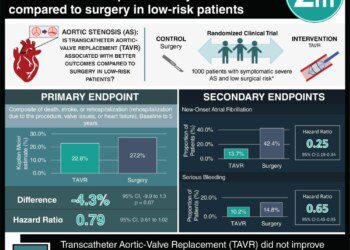
Transcatheter Aortic-Valve Replacement with a Self-Expanding Prosthesis
Although aortic valve replacement (AVR) is the only definitive treatment for aortic stenosis, patients with the condition area also often considered high-risk for surgical AVR. In this multicenter, randomized noninferiority trial, 795 patients with severe aortic stenosis, New York Heart Association class 2 or higher heart failure symptoms, and increased risk for surgical AVR (estimated risk of death within 30 days of surgery 15% to 50%) were randomized to transcatheter AVR (TAVR) with a self-expanding prosthesis or conventional surgical open-heart AVR in order to determine rate of mortality from any cause at 1 year. One-year mortality in the TAVR group (n=390) was lower (14.2%) than in the surgical group (19.1%, p<.001 for noninferiority, p=.04 for superiority). Even though rates of moderate or severe paravalvular regurgitation were higher in the TAVR group (6.1% vs 0.5%, p<.001), they were lower than described in previous trials, and did not affect overall mortality. TAVR was found to be noninferior to surgical AVR for most secondary endpoints as well, including change in aortic valve gradient (-39.04 vs -35.42mmHg, p<.001), symptomatic improvement (p<.01), and risk of cardiovascular or cerebrovascular events at 1 year (20.4% vs 27.3%, p=.03). There was no difference in stroke rates between the two groups at 30 days or 1 year (TAVR 4.9% vs 6.2% in the surgical group at 30 days, p=.46; 8.8% vs 12.6% at 1 year, p=.10). Rate of death at 1 year was substantially reduced with a transcatheter self-expanding prosthesis compared to open-heart valve replacement in patients with aortic stenosis considered to be at increased surgical risk.
Two approaches to transcatheter aortic valve replacement (TAVR) have both been shown to be effective options for patients with aortic stenosis who are considered high-risk for traditional surgical valve replacement: balloon-expandable and self-expandable valves. They have not been compared directly in randomized studies. In this randomized multicenter trial in Germany, 241 patients with severe aortic stenosis, New York Heart Association class 2 or higher heart failure symptoms, high risk of surgical valve replacement, and native aortic valve annulus of 20-27mm in diameter were randomized to transfemoral TAVR using the balloon-expandable valve or the self-expandable valve to determine device success (successful deployment, correct placement, minimal paravalvular regurgitation). Device success was higher in the balloon-expandable valve group than the self-expandable valve group (95.9% vs 77.5%, RR 1.24, 95%CI 1.12-1.37, p<.001). Fewer patients receiving balloon-expandable valves required a second valve due to mispositioning (0.8% vs 5.8%, p=.03), and required postdilatation due to aortic regurgitation less frequently than the self-expandable valve group (19.8% vs 49.2%, p<.001). Moderate to severe paravalvular regurgitation at 30 days was lower in the balloon-expandable group valve group (0.0% vs 7.2%, p=.009), though the transvalvular gradient was slightly higher (8.9mmHg vs 6.6mmHg, p<.001). The balloon-expandable valve group also had fewer rehospitalizations for heart failure at 30 days (p=.02), required fewer pacemaker placements (17.3% vs 37.6%, p<.001), and reported higher quality of life (p=.02), though mortality at 30 days was similar between groups (p=.77), and there were similar rates of stroke, vascular complications, and bleeding.
© 2012-2014 2minutemedicine.com. All rights reserved. No works may be reproduced without written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT. Content is produced in accordance with fair use copyrights solely and strictly for the purpose of teaching, news and criticism. No benefit, monetary or otherwise, is realized by any participants or the owner of this domain.
RelatedReports





{kind=link}
