
Nirmatrelvir–ritonavir does not improve severe outcomes in adults vaccinated against COVID-19
1. In two large randomized platform trials, early treatment with nirmatrelvir–ritonavir did not reduce hospitalization or death among mostly vaccinated, higher-risk outpatients with COVID-19.
2. Treatment was associated with faster symptom recovery and reduced viral load, though adverse effects (e.g., dysgeusia, gastrointestinal symptoms) were common.
Evidence Rating Level: 1 (Excellent)
Study Rundown: As population-level immunity to SARS-CoV-2 has increased through vaccination and prior infection, the baseline risk of severe COVID-19 outcomes has declined, raising uncertainty about the continued benefit of antiviral therapies initially proven effective in unvaccinated populations. In this context, two randomized controlled trials conducted in the United Kingdom and Canada evaluated whether nirmatrelvir–ritonavir improves outcomes in higher-risk community-dwelling adults in the modern, largely immunized era. In analysis of both trials, early outpatient treatment did not meaningfully reduce the already low rates of hospitalization or death when compared with usual care. However, patients receiving antiviral therapy experienced faster self-reported recovery and demonstrated reductions in viral load, suggesting ongoing biologic activity despite limited impact on severe endpoints. These findings highlight a shift in therapeutic value from preventing severe disease toward potentially shortening illness duration. Strengths of the study include its pragmatic design and high generalizability to current clinical settings. The inclusion of predominantly vaccinated individuals enhances its relevance to present-day practice. However, limitations include the open-label design, which may influence subjective outcomes such as symptom reporting, and lower-than-expected event rates, which reduced statistical power to detect differences in severe outcomes. Additionally, some heterogeneity existed between the two trials in follow-up and recruitment timing. Nonetheless, this study demonstrated that nirmatrelvir–ritonavir did not significantly affect severe outcomes of COVID-19 infection.
Click to read the study in NEJM
Relevant Reading: Effectiveness of nirmatrelvir/ritonavir and molnupiravir in non-hospitalized adults with COVID-19: systematic review and meta- analysis of observational studies.
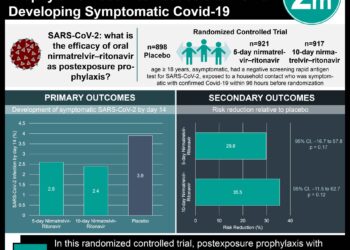
In-Depth [randomized controlled trial]: This study evaluated the effectiveness of nirmatrelvir–ritonavir in two open-label, randomized platform trials: PANORAMIC in the United Kingdom and CanTreatCOVID in Canada. Eligible participants were non-hospitalized adults at increased risk for severe COVID-19 (older age or comorbidities) who had experienced symptoms for five days or less. Importantly, the vast majority of participants had received prior COVID-19 vaccination, reflecting a contemporary, immunized population. Individuals were randomized to receive usual care alone or usual care plus a five-day course of oral nirmatrelvir–ritonavir. The primary endpoint was a composite of hospitalization or death from any cause within 28 days. In the PANORAMIC trial, hospitalization or death occurred in 14 of 1698 participants (0.8%) in the treatment group compared with 11 of 1673 (0.7%) in the usual-care group (adjusted odds ratio [OR], 1.18; 95% Bayesian credible interval [CrI], 0.55 to 2.62). In the CanTreatCOVID trial, events occurred in 2 of 343 participants (0.6%) receiving treatment versus 4 of 324 (1.2%) receiving usual care (adjusted OR, 0.48; 95% CrI, 0.08 to 2.23). Secondary outcomes suggested clinical benefit in symptom resolution. In PANORAMIC, early sustained recovery occurred in 33.0% of treated participants versus 22.1% with usual care (adjusted OR, 1.74; 95% CrI, 1.48 to 2.04), with a shorter median time to recovery (14 vs. 21 days). Similarly, in CanTreatCOVID, recovery by day 14 was higher with treatment (69.0% vs. 53.1%; adjusted OR, 1.99; 95% CrI, 1.40 to 2.87), with a shorter median recovery time (6 vs. 9 days). A virologic substudy in PANORAMIC demonstrated lower SARS-CoV-2 viral loads at day 5 in the treatment group (geometric mean ratio, 0.13; 95% CrI, 0.08 to 0.21), supporting a biological effect. Adverse events were common with nirmatrelvir–ritonavir, particularly dysgeusia and gastrointestinal symptoms, but serious adverse events were rare overall.
Image: PD
©2026 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports



![Shorter moxifloxacin-containing regimens ineffective for treating TB [REMoxTB trial]](https://www.2minutemedicine.com/wp-content/uploads/2014/09/TB-original-e1591582219420-75x75.jpg)
![2 Minute Medicine: Pharma Roundup: Price Hikes, Breakthrough Approvals, Legal Showdowns, Biotech Expansion, and Europe’s Pricing Debate [May 12nd, 2025]](https://www.2minutemedicine.com/wp-content/uploads/2025/05/ChatGPT-Image-May-12-2025-at-10_22_23-AM-75x75.png)

{kind=link}
