
Patient Basics: Colorectal Cancer
Originally published by Harvard Health.
What Is It?
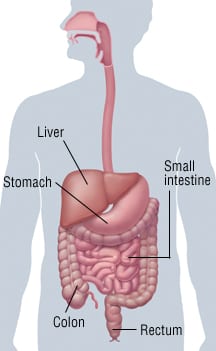
Colorectal cancer is an uncontrolled growth of abnormal cells in the colon and/or rectum.
Together, the colon and rectum make up the large intestine. The large intestine carries waste from the small intestine and eliminates it through the anus.
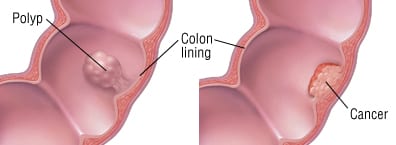
Colorectal tumors often begin as small growths (polyps) on the inside of the large intestine. Polyps that are not removed eventually can become cancerous.
Risk Factors
Risk factors for colorectal cancer include:
- Increasing age
- Family history of colorectal cancer
- Personal history of colorectal cancer
- Personal history of polyps
- Inflammatory bowel disease, including persistent ulcerative colitis and Crohn’s disease
- Diet low in fiber and high in saturated fat
- Sedentary lifestyle
- Race and ethnicity (Alaska natives have the highest risk)
Symptoms
Polyps and early colorectal cancer generally don’t cause symptoms. As a result, they are usually caught during screening.
More advanced cancer can cause:
- More or less frequent bowel movements than usual
- Diarrhea or constipation
- Blood in the stool (bright red, black or very dark)
- Narrowed stools (about the thickness of a pencil)
- Bloating, fullness or stomach cramps
- Frequent gas pains
- A feeling that the bowel does not empty completely
- Weight loss without dieting
- Continuing fatigue
Diagnosis
If your doctor suspects colorectal cancer, he or she will perform a sigmoidoscopy or colonoscopy. This is done with an instrument called a scope. A scope is a flexible tube with a camera attached at one end. The doctor inserts the scope into your rectum and colon to look for polyps or cancer.
In some cases, your doctor may recommend a biopsy. A doctor or surgeon removes a small piece of tissue to be examined in a laboratory.
Your doctor may also perform other imaging and laboratory tests. These may include x-rays, computed tomography (CT) scans, and blood tests.
Expected Duration
Without treatment, colon cancer will continue to grow.
Prevention
The best defense against colorectal cancer is regular screening. Screening tests are designed to find polyps so they can be removed before they become cancerous.
The American Cancer Society recommends that all adults begin screening at age 50. People at higher risk should begin screening earlier. You are at high risk if you:
- Have been diagnosed with polyps before age 50.
- Have inflammatory bowel disease, including ulcerative colitis and Crohn’s disease.
- Have a genetic disorder that increases your likelihood of developing colorectal cancer.
- Have one or more first degree relatives (a parent or sibling) diagnosed with colon cancer before age 50.
Recommended screening methods include:
- Digital rectal examination. Your doctor inserts a gloved finger into your anus to check for abnormal lumps or masses. This should not be used as the only screening method.
- Fecal occult blood test. This test detects small amounts of blood in the stool. However, blood in the stool does not necessarily mean you have colon cancer.
- Sigmoidoscopy. The doctor uses a scope to examine the rectum and part of the colon.
- Colonoscopy. The doctor uses a scope to examine your entire colon and rectum.
- Virtual colonoscopy. Images of the colon are taken with computed tomography (CT) scans.
Daily exercise and a diet low in saturated fat may lower your risk of colorectal cancer.
Taking aspirin or folate every day may also reduce your risk. Talk to your doctor to see if this is appropriate for you.
Treatment
Surgery is the main treatment for colorectal cancer. You may also have chemotherapy or radiation.
The extent of surgery and whether you need treatment after surgery depends on:
- Whether the cancer is in the colon or rectum.
- The stage of the disease. The cancer’s stage depends on how far the cancer has spread.
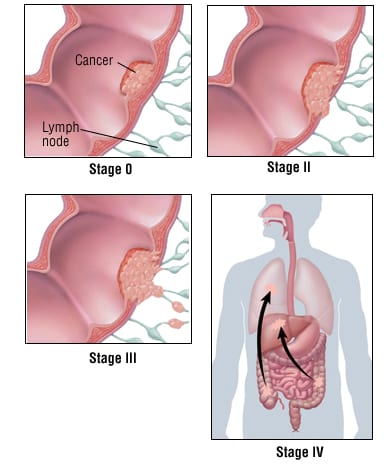
Following are the stages of colorectal cancer, along with recommendations for treatment in addition to surgery:
- Stage 0. Cancer remains within the inner layer of the colon or the rectal lining. Your doctor is unlikely to recommend any treatment, except for additional, regular follow up, after surgery to remove polyps or cancer.
- Stage I. Cancer has grown through the inner rectal wall or the inner lining of the colon and the underlying layers. It has not broken through the colon wall. Usually, no treatment is recommended after surgery.
- Stage II. Cancer has grown through the colon or rectal wall. It has not spread to nearby lymph nodes. The doctor may recommend chemotherapy after surgery in some cases of colon cancer. For rectal cancer, chemotherapy and radiation can be used before or after surgery.
- Stage III. Cancer has spread to nearby lymph nodes but not to other parts of the body. For colon cancer, chemotherapy typically is recommended after surgery. For rectal cancer, chemotherapy and radiation usually are given before or after surgery.
- Stage IV. Cancer has spread to distant organs. Treatment after surgery consists of chemotherapy, radiation therapy or both to relieve the symptoms of advanced cancer and, in rectal cancer, to prevent the blockage of the rectum. Occasionally, surgery is needed to remove cancer from the sites where it has spread.
Colon Cancer
Surgery for colon cancer removes the cancerous area of the colon, some surrounding normal tissue and nearby lymph nodes.
Recovery time depends on several factors, including the person’s age, general health and the extent of the surgery.
Rectal Cancer
Treatment for rectal cancer often combines surgery with chemotherapy and radiation, which can be given before or after surgery.
Early stage rectal cancer may only require removal of polyps. Late stage rectal cancer may require removal of the rectum, anus, and part of the colon.
In some cases of late-stage surgery, the surgeon must reroute the colon through a hole in the abdomen to create a new way for the body to eliminate waste. This is called a colostomy.
When to Call a Doctor
Visit a doctor for regular colorectal cancer screening. Also, see your doctor if you have any signs or symptoms of colorectal cancer.
Prognosis
The outlook for colorectal cancer depends on the stage of the disease. Nearly everyone with stage 0 cancer will survive 5 years or more. The outlook is less favorable for people with stage IV cancer.
Additional Info
American Cancer Society (ACS)
Toll-Free: 1-800-227-2345
TTY: 1-866-228-4327
Cancer Research Institute
National Headquarters
One Exchange Plaza
55 Broadway, Suite 1802
New York, NY 10022
Toll-Free: 1-800-992-2623
http://www.cancerresearch.org/
Centers for Disease Control and Prevention (CDC)
1600 Clifton Road
Atlanta, GA 30333
Phone: 404-639-3534
Toll-Free: 1-800-311-3435
National Cancer Institute (NCI)
NCI Public Inquiries Office
6116 Executive Blvd.
Room 3036A
Bethesda, MD 20892-8322
Toll-Free: 1-800-422-6237
TTY: 1-800-332-8615
RelatedReports


![2MM: AI Roundup- AI Cancer Test, Smarter Hospitals, Faster Drug Discovery, and Mental Health Tech [May 2nd, 2025]](https://www.2minutemedicine.com/wp-content/uploads/2025/05/Untitled-design-350x250.png)




