




{kind=link}


Coronary CT angiography not superior to functional testing in cardiac risk management [Classics Series]
This study summary is an excerpt from the book 2 Minute Medicine’s The Classics in Medicine: Summaries of the Landmark Trials
1. Computed tomographic coronary angiography (CTCA) as the initial diagnostic test for patients at intermediate risk of coronary artery disease (CAD) was not superior to functional cardiac testing with regard to all-cause mortality or major cardiovascular events over a 2-year period.
2. Patients in the CTCA group underwent significantly more cardiac catheterizations (though with fewer procedures revealing no CAD) and subsequently had an increased rate of coronary revascularization than those in the functional testing arm.
Original Date of Publication: April 2015
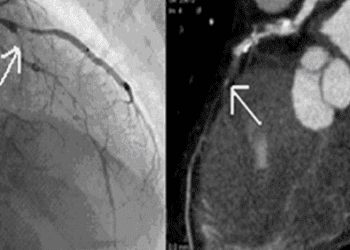
Study Rundown: BPatients with suspected CAD, such as those with new-onset stable angina or at least one major cardiac risk factor, require diagnostic testing to determine both their burden of disease and the appropriateness of medical or surgical intervention in cardiac risk mitigation. Noninvasive testing for CAD is indicated for such intermediate-risk, ambulatory patients and has historically involved a functional test, such as a stress electro- or echocardiogram or a nuclear stress test, any of which can reveal indirect evidence of CAD if reversible ischemia is present. However, CTCA has emerged as a viable alternative to functional testing with a theoretically increased specificity given that it provides a direct anatomical assessment. It has even been proposed that CTCA may reveal nonobstructive but prognostically significant coronary lesions. The Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE) randomized outpatients with new onset, stable chest pain or with at least one major cardiac risk factor to either CTCA or functional testing for CAD in an effort to determine if noninvasive anatomical testing might improve cardiac outcomes over functional testing. Over the 2-year follow-up period from initial randomization, no significant differences were found in all-cause mortality or major cardiovascular events between the two groups, though patients in the CTCA group underwent an increased rate of cardiac catheterization and subsequent surgical or percutaneous coronary revascularization. Notably, the study was not designed or powered to assess, given its relatively short length of follow-up, if the observed increased rate of catheterization and revascularization might have affected long-term outcomes. Within this limitation, PROMISE established that CTCA is not superior to standard functional cardiac testing in the initial workup of patients at intermediate risk of CAD. However, future trials are necessary to determine if the increased rate of revascularization observed within the CTCA group may yield a longitudinal mortality benefit.
Click to read the study in NAJM
In-Depth [randomized controlled trial]: A total of 10 003 outpatients (mean age 60±8.3 years, 52.7% women) presenting primarily with new onset, stable chest pain without a prior diagnosis of CAD were enrolled at several major medical centers across the United States. Patients were randomized to either undergo CTCA or functional cardiac testing for the non-urgent, non-invasive workup of suspected CAD, and were followed for a median period of 25 months. Functional tests utilized in the control arm of the trial included nuclear stress testing (67.5%), stress echocardiography (22.4%), and exercise electrocardiography (10.2%). The primary endpoints of the trial were all-cause mortality or major cardiovascular events (including complications from diagnostic or therapeutic cardiovascular procedures), while secondary endpoints included invasive cardiac catheterizations, particularly those that did not reveal CAD, and cumulative radiation exposure. Median cumulative radiation exposure was lower per patient in the CTCA group than the functional testing group (10.0 mSv versus 11.3 mSv; p <0.001). The bulk of per patient exposure occurred secondary to nuclear stress testing, though overall exposure was greater within the CTCA group as 32.6% of patients in the functional testing group had no radiation exposure. The study was powered at 90% confidence to detect a 20% relative reduction in the primary endpoint between groups assuming an overall event rate of 8% at 2.5 years post-randomization. The true observed overall event rate was 3.1% for mortality or major cardiovascular events, with no significant difference between the CTCA group (3.3%) and the functional testing group (3.0%; adjusted hazard ratio 1.04; 95%CI 0.83-1.29; p = 0.075) over the median 25-month follow-up period. A similar rate of positive initial tests was observed between the two groups, with 10.7% of initial CTCAs and 11.7% of functional tests interpreted as positive. In the 90 days following randomization, 12.2% of patients in the CTCA group underwent cardiac catheterization as opposed to only 8.1% of the functional testing group, but catheterizations performed in the CTCA group significantly more likely to be positive (72.1% versus 52.5%; p = 0.02). Additionally, revascularization (either surgical or percutaneous) was significantly more commonly performed within the CTCA group, occurring in 6.2% of patients as compared to 3.2% in the functional testing group (p <0.001). However, revascularization was not a trial end point, and the study was not adequately powered to assess the effect of this difference on long-term cardiovascular outcomes.
Douglas PS, Hoffmann U, Patel MR, Mark DB, Al-Khalidi HR, Cavanaugh B, et al. Outcomes of anatomical versus functional testing for coronary artery disease. The New England Journal of Medicine. 2015 Apr 2;372(14):1291–1300.
©2022 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
