




{kind=link}


Antibiotic GBS prophylaxis linked to decreased early-onset neonatal infection [Pediatrics Classics Series]
Image: PD
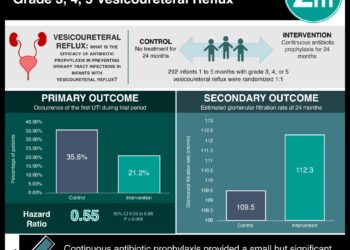
1. During the 1990-1998 study period, which included the 1996 initiation of national Group B Streptococcus guidelines, a significant, 65% decrease in early-onset neonatal disease was observed.
2. During the study’s final year, an estimated 3900 early-onset neonatal GBS cases along with 200 early- and late-onset neonatal deaths were believed to have been prevented through the use of recommended antibiotic prophylaxis.
Original Date of Publication: January 2000
Study Rundown: With the identification of Group B Streptococcus (GBS) as a pathogen leading to significant neonatal morbidity and mortality secondary to maternal transmission, the United States instituted a national advocacy group and guideline recommendations to prevent and manage perinatal GBS infection during the 1990s. This study was the first to assess trends in GBS disease following the issuance of 1996 American Academy of Pediatrics(AAP)-, American College of Obstetricians and Gynecologists-, and Centers for Disease Control (CDC)-approved guidelines instructing practitioners on how to effectively use intrapartum antibiotic prophylaxis. Based on high transmission risk or positive 35-37 week screening, women were instructed to receive intrapartum antibiotics. Researchers found a significant, 65% reduction in GBS early-onset neonatal disease, defined as disease manifesting before 7 days of life, but no difference in neonatal disease diagnosed at 7-89 days of life. When these findings were projected upon 1998 national data, it was believed that about 3900 early-onset cases and 200 deaths due to neonatal GBS infection had been prevented by the guideline issuance. A significant, 21% reduction in GBS disease among pregnant women and girls was also seen. This study is limited in its generalizability due to lack of racial diversity, particularly in its low numbers of Hispanic participants and in the likely higher alertness of practitioners in the study to GBS positivity. However, this large, multi-state study did allow for assessment of the guidelines among many laboratory-confirmed GBS cases. With this research indicating the effectiveness of preventative strategies in decreasing early-onset neonatal GBS infection, continued efforts to promote prevention, appropriate antibiotic intervention, and to determine why these strategies fail was and still are necessary. Antibiotic resistance, lack of education, and decreased compliance were indicated as potential contributors to unsuccessful prevention and continue to be problematic today. The 1996 guidelines were later updated by the CDC in 2010 and an AAP policy statement followed in 2011. Both are available at the links below. The guidelines continue to be updated in order to improve case detection, while reducing false positives.
Click to read the study in The New England Journal of Medicine
Click to read the current guidelines (last updated 2010)
Click to read the most recent AAP policy statement published in Pediatrics in 2011
In-Depth [cross-sectional study]: During 1993 to 1998, GBS cases in Maryland, California, Georgia, Tennessee, Connecticut, Minnesota, Oregon, and New York were reported through a laboratory-based surveillance protocol. Additional data from California, Georgia, and Tennessee for 1990-1993 were included to provide a greater temporal context for GBS rates prior to guideline initiation. GBS cases were reported if individuals tested positive for GBS in normally sterile body fluid. GBS isolated from either placenta, amniotic fluid, or urine was not included. GBS disease was classified by time of onset as follows: early-onset neonatal disease (< 7 days old), late-onset (7-89 days old), childhood disease (90 days to 14 years of age), adult disease as (> 15 years old). Disease in pregnancy was considered separately. National estimates of GBS incidence were calculated based on known population sizes.
During the 5-year study period, 7867 GBS cases were reported (84% from blood, 4% from cerebrospinal fluid, 4% from joint fluid, and the remainder from other sites). GBS disease incidence and mortality by age is reported in the table below. Early-onset disease remained constant throughout 1990-1993 and then declined by a significant 65% during 1993-1998 (1.7 per 1000 births in 1993 v. 0.6 per 1000 in 1998, X2 = 121.0, p < 0.001). African Americans had higher early-onset disease rates, but also underwent a steeper reduction during the study period than whites, with a 75% reduction in the difference between the two groups by 1998. No significant change in late-onset disease incidence took place in 1990-1998. Among pregnant women and girls, a significant, 21% reduction in GBS incidence was seen over the study course (0.29 per 1000 births in 1993 v. 0.23 per 1000 births in 1998, X2= 4.86, p < 0.03). After projecting 1998 incidence from the selected states onto national data, it was estimated 3900 neonatal early-onset GBS cases and 200 early- and late-onset neonatal deaths were prevented through antibiotic usage.
Table. GBS cases and mortality by age during 1993-1998. Adapted from Shrag et al.
| Age at GBS diagnosis | GBS case (% total cases) | Mortality rate (%) |
| Early-onset neonatal (< 7 days old) | 1584 (20) | 4.7 |
| Late-onset neonatal (7-89 days old) | 612 (8) | 2.8 |
| Childhood disease (90 days to 14 years old, not pregnant) | 175 (2) | 9.0 |
| Adult disease (15-64 years old, not pregnant) | 2559 (33) | 8.0 |
| Adult disease at > 65 years old | 2559 (333) | 15.0 |
| Pregnant individuals | 345 (4) | 0.003 |
© 2014 2minutemedicine.com. All rights reserved. No works may be reproduced without expressed written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors, editors, staff or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT.
RelatedReports
