
Cardiac Resynchronization Therapy may be more beneficial in women
1. In patients with left bundle-branch block (LBBB) and QRS duration of 130-149 milliseconds (ms), women had a significant reduction in the end-point of heart failure and death, while men had no significant benefit, when receiving CRT-defibrillator (CRT-D) therapy.
2. Neither sex benefited from CRT-D therapy if they had a LBBB and QRS duration less than 130ms.
Evidence Rating Level: 2 (Good)
Study Rundown: Several previous trials have demonstrated the benefits of improved heart failure symptoms and mortality in heart failure patients receiving CRT therapy. As in other device trials, women were underrepresented in these trials as well. The 2012 guideline were revised, giving a class I indication for CRT to patients with LBBB and QRS≥150ms. As these guidelines were based on study-level meta-analyses that have the disadvantage of not being able to study sex differences due to the lack of individual patient data, this study pooled individual patient-data from 3 large randomized clinical trials comparing CRT-D to implantable cardioverter defibrillator (ICD) therapy.
The study found that women seemed to derive more benefit from CRT-D than men. Women seem to derive this benefit if they had a LBBB and QRS duration greater than 130ms. Men did not have a significant benefit at this duration. Also, both groups saw no benefit if they had a LBBB but QRS was less than 130ms and saw a benefit if QRS was greater than 150ms. Strengths of the study include the large number of patients for whom patient level data was analyzed. Of note, this study examined data from studies that mostly enrolled patients with NYHA class II heart failure symptoms. Therefore, these conclusions cannot be applied to patients with class III or IV symptoms. Although randomized clinical trials provide the best data, they can be expensive and can require very large numbers of patients to derive any meaningful conclusions. This study highlights the importance of data mining from existing trials to add to our understanding of device therapies. Along the same tangent, data from registries and post-approval trials can also help us refine indications for devices in a much more efficient manner.
Click to read the study, published today in JAMA Internal Medicine
Relevant Reading: 2012 ACCF/AHA/HRS Focused Update of the 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities
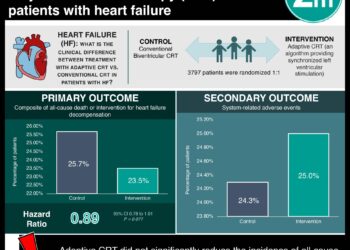
In-Depth [meta-analysis]: The authors decided to collect and analyze patient-level data from randomized clinical trials comparing CRT-D to ICD in patients with Class II CHF symptoms. Three trials met their criteria: MADIT-CRT, RAFT, and REVERSE trials. Data from 4076 patients from these three trials with class II symptoms and follow-up to 3 years was collected. The primary outcome was time to heart failure event or death and the secondary outcome was death.
Overall, in women, CRT-D resulted in a 60% relative risk reduction (RRR) in heart failure or death and 55% RRR in death. In men, there was a 26% and 15% RRR in the same end-points respectively. In patients with LBBB and QRS duration between 130-149ms, CRT-D did not have a significant impact in men while in women there was 76% RRR (HR, 0.24 [95%CI, 0.11-0.53]) in the primary end-point and a 76% RRR in death (HR, 0.24 [95%CI, 0.06-0.89]).
Image: PD
©2012-2014 2minutemedicine.com. All rights reserved. No works may be reproduced without expressed written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors, editors, staff or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT.
RelatedReports
![Adverse pregnancy outcomes associated with thrombophilias [Classics Series]](https://www.2minutemedicine.com/wp-content/uploads/2015/07/Classics-2-Minute-Medicine-e1436017941513-350x250.png)



{kind=link}
