
Flexible ICU family visits not effective at reducing delirium incidence
1. In this randomized controlled trial, there was no difference in the incidence of delirium between flexible family visitation and standard, restricted family visitation.
2. Flexible visitation resulted in better measures of anxiety, depression, and satisfaction for family members.
Evidence Rating Level: 1 (Excellent)
Study Rundown: It is thought that flexible ICU visiting hours may contribute to delirium prevention and stress reduction among patients as well as improvement in family satisfaction. While some professional society guidelines have recommended flexible visitation policy for family members in ICUs, it is unclear if this would reduce delirium. In this cluster-crossover randomized clinical trial, flexible family visitation did not reduce the incidence of delirium compared to standard, restricted family visitation. However, flexible visitation resulted in better measures of anxiety, depression, and satisfaction for family members.
This study has several limitations. First, all the ICUs studied were from a single country, and flexible visitation may have different effects across distinct sociocultural contexts and cultures. In addition, cluster randomization was susceptible to recruitment bias. Lastly, the effect of the educational component of the flexible visitation model on family members cannot be isolated from flexible visiting hours.
Click to read the study in JAMA
Relevant Reading: The effectiveness of interventions to meet family needs of critically ill patients in an adult intensive care unit: a systematic review update.
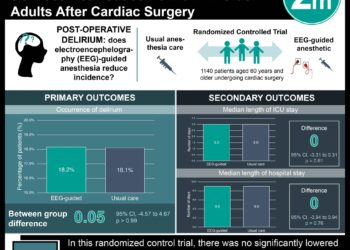
In-Depth [randomized controlled trial]: As part of the larger ICU Visits Study, this cluster-crossover randomized clinical trial recruited 1685 patients, family members, and clinicians from 36 adult ICUs with restricted visiting hours (<4.5 hours per day) in Brazil. Patients were divided between flexible visitation (up to 12 hours per day) supported by family education or usual restricted visitation (median, 1.5 hours per day). The primary outcome was incidence of delirium during ICU stay, assessed using the CAM-ICU. Secondary outcomes included ICU-acquired infections for patients; symptoms of anxiety and depression assessed using the HADS (range, 0 [best] to 21 [worst]) for family members; and burnout for ICU staff (Maslach Burnout Inventory). There was no significant difference in the primary outcome between the interventions: delirium occurred in 18.9% in the flexible visitation group and in 20.1% in the restricted visitation group (risk ratio 0.91; CI95, 0.73 to 1.15). Flexible visitation effects were not significantly different from restricted visitation effects for daily hazard of delirium (0.09 vs 0.10; hazard ratio 0.88; CI95, 0.74 to 1.04), incidence of ICU-acquired infections (3.7% vs 4.5%; RR 0.81; CI95, 0.51 to 1.29), mean 7-day ventilator-free days (5.9 vs 6.0; adjusted difference −0.01 days; CI95, −0.05 to 0.03), median days of ICU stay (5.0 vs 5.0; adjusted difference −0.02 days; CI95, −0.15 to 0.09), and hospital mortality (14.8% vs 14.4%; RR, 1.01; CI95 0.77 to 1.32). In family members, flexible visitation resulted in significantly better median scores for HADS anxiety (6.0 vs 7.0; adjusted difference, −1.6 points; CI95 −2.3 to −0.9) and HADS depression (4.0 vs 5.0; adjusted difference −1.2 points; CI95, −2.0 to −0.4) and mean scores for CCFNI satisfaction (146.1 vs 132.6; adjusted difference 13.5 points; CI95, 10.4 to 16.7]) compared with restricted visitation.
Image: PD
©2019 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.






{kind=link}