
Intraarterial therapy and t-PA increase reperfusion and functional independence after acute ischemic stroke [Classics Series]
This study summary is an excerpt from the book 2 Minute Medicine’s The Classics in Medicine: Summaries of the Landmark Trials
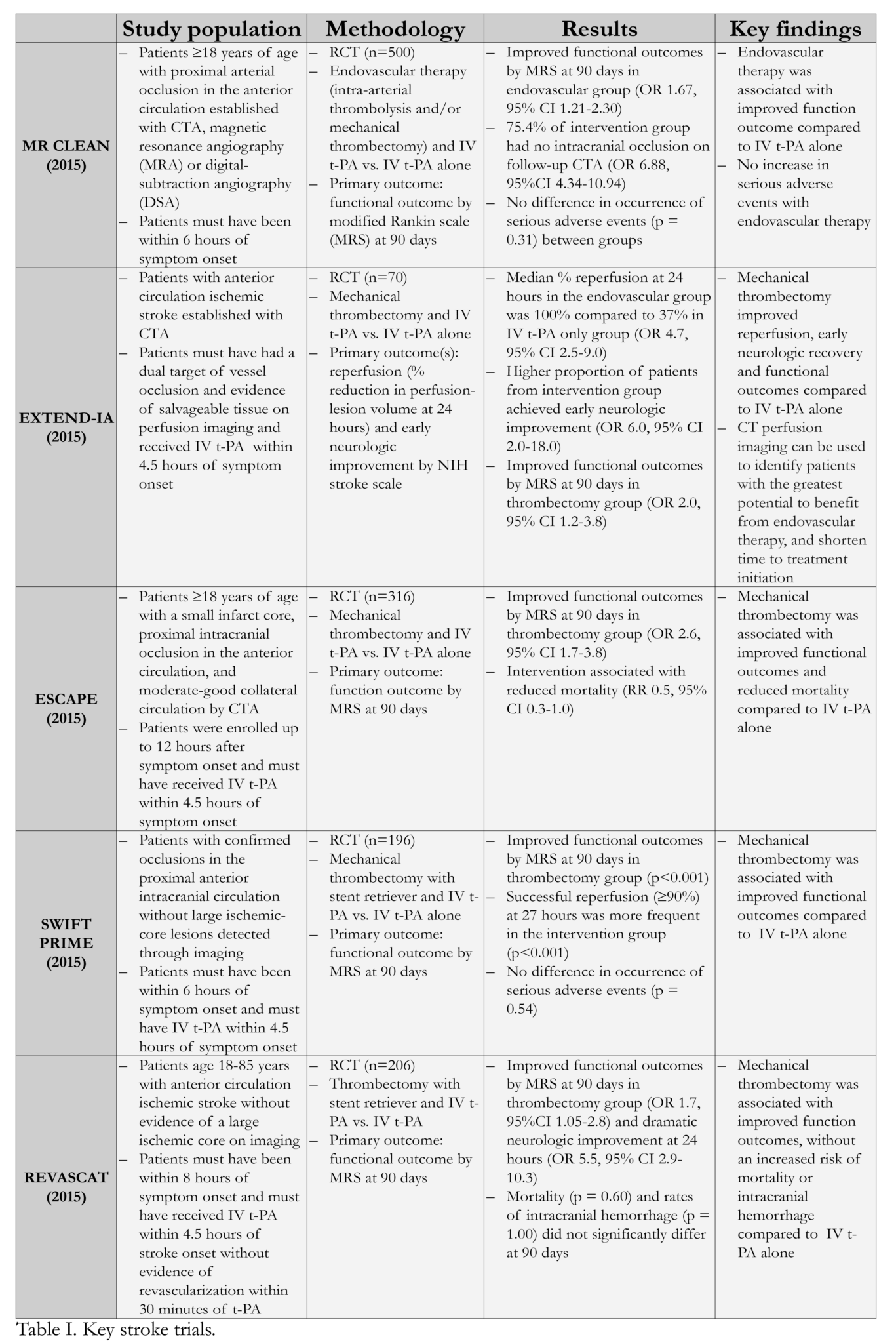
1. Across several randomized controlled trials (Table I), patients treated with intraarterial therapy and intravenous (IV) tissue plasminogen activator (t-PA) had consistently improved functional outcomes compared to patients that received IV t-PA alone.
2. Patients were more likely to achieve successful reperfusion after receiving both intraarterial and medical therapy.
3. The addition of intraarterial therapy to usual care did not increase rates of mortality or serious adverse events.
Original Dates of Publication: Multiple 2015 Trials
Study Rundown: The intravenous (IV) administration of alteplase, a tissue plasminogen activator (t-PA) involved in the breakdown of blood clots, has long been the mainstay in treating acute ischemic stroke. However, a narrow therapeutic time window and various contraindications (i.e. recent surgery, coagulation abnormalities, history of intracranial hemorrhage) have limited the number of patients who qualify for t-PA therapy. IV alteplase is also less effective in penetrating through proximal occlusions of major intracranial arteries, which account for over a third of acute anterior-circulation strokes. Intraarterial therapy includes the chemical dissolution of clots with locally delivered thrombolytic agents and/or clot retrieval through thrombectomy with mechanical devices. While a number of trials have been conducted to evaluate the efficacy of intraarterial therapy compared to more conventional treatment, concerns surrounding the design and execution of these studies left uncertainty on the role of intraarterial therapy in managing acute ischemic stroke in conjunction with alteplase.
As part of the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN), patients with proximal arterial occlusion in the anterior cerebral circulation received intraarterial treatment with usual care or usual care alone. Berkhemer and colleagues found that at 90 days of follow-up, patients that received intraarterial therapy in addition to usual care had significantly improved functional outcomes. The results of computed tomography angiography (CTA) also showed that after 24 hours, patients assigned to the intervention group were significantly less likely to have residual occlusion. There were no significant differences in the occurrence of serious adverse events; however, a higher proportion of patients from the interventional group demonstrated clinical signs of a new ischemic stroke in a different vascular territory. Given the invasive nature of intraarterial therapy, these patients were also subject to procedure-related complications not seen in the control group.
Campbell and colleagues subsequently conducted the Emergency Neurological Deficits – Intra-Arterial (EXTEND-IA) trial to evaluate whether the use of computed tomographic (CT) perfusion imaging could be used in maximizing the therapeutic potential of intraarterial interventions. Specifically, CT perfusion imaging was used to identify patients with a dual target of vessel occlusion and evidence of salvageable tissue; patients with large ischemic cores and without evidence of clinically significant salvageable ischemic brain tissue were not included in the study. Unlike the MR CLEAN trial where various forms of intraarterial therapy were employed, patients in this study received intraarterial therapy using a stent retriever and IV alteplase, or alteplase alone within 6 hours of stroke onset. As the results of an interim analysis strongly favored the intervention, this trial was stopped early, demonstrating that CT perfusion imaging can be effectively used to identify patients with the greatest potential to benefit from endovascular therapy. Specifically, early combination endovascular therapy and IV alteplase was associated with significantly earlier neurologic improvement when compared to the receipt of IV alteplase alone. Patients in the intervention group also achieved greater overall reperfusion after 24 hours, corresponding to improved functional outcomes measured at 90 days. The use of CT perfusion imaging also shortened the time to treatment initiation. The results of this study were echoed in the Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times (ESCAPE) trial published in the same issue of The New England Journal of Medicine (NEJM).
Like the EXTEND-IA trial, patients in the ESCAPE trial were initially evaluated using CT and CTA, and considered eligible if they had a small infarct core, an occluded proximal artery in the anterior circulation, and moderate-to-good collateral circulation. Unlike the ESCAPE trial, however, enrollment up to 12 hours after the onset of stroke symptoms was permitted, and intraarterial therapy was not restricted to the use of retrievable stents. As this study was also terminated early, results reflected that of an interim analysis, where the intervention was significantly favored with respect to improved functional outcomes. The mortality rate among patients that received both intraarterial therapy and IV alteplase was also significantly decreased when compared to patients that received alteplase alone, and rates of symptomatic intracerebral hemorrhage did not significantly differ. The median time from initial imaging to groin puncture and median time to first visualization of reflow in the middle cerebral artery in the intervention group were also considerably reduced compared to previous studies, including the EXTEND-IA trial.
Less than six months after the release of the EXTEND-IA and ESCAPE trials, the results of the Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME) emerged. Using similar methodology to the EXTEND-IA and ESCAPE studies, namely strict imaging eligibility requirements, Saver and colleagues further confirmed that patients receiving IV t-PA and thrombectomy using a stent retriever had significantly better functional outcomes at 90 days, with the proportion of patients achieving functional independence far exceeding that observed in patients that received t-PA alone. The proportion of patients with successful reperfusion in the intervention group was also twice as high as that seen in the control group, without significantly increasing the risk of serious adverse events or 90-day mortality. This study also noted that patients who received IV t-PA at another hospital before being transferred to a study site for thrombectomy had less favorable outcomes, where levels of functional independence in these patients did not significantly from that observed in patients receiving t-PA alone.
The REVASCAT study also reiterated the value of administering combination intraarterial and medical therapy. Like the prior studies, following visualization of an occlusion in the proximal anterior circulation without a large core, patients were randomized to receive thrombectomy using a stent retriever and medical therapy or medical therapy alone. Consistent with the aforementioned studies, patients in the intervention group had significantly improved functional outcomes compared to those that received medical therapy alone. Patients that received intraarterial therapy were also significantly more likely to exhibit dramatic neurologic improvements at 24 hours, without an increase in the risk of experiencing serious adverse events or death.
Click to read the MR CLEAN study in NEJM
Click to read the EXTEND-IA study in NEJM
Click to read the ESCAPE study in NEJM
Click to read the SWIFT PRIME study in NEJM
Click to read the REVASCAT study in NEJM
 Berkhemer OA, Fransen PSS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke. The New England Journal of Medicine. 2015 Jan;372(1):11-20.
Berkhemer OA, Fransen PSS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A Randomized Trial of Intraarterial Treatment for Acute Ischemic Stroke. The New England Journal of Medicine. 2015 Jan;372(1):11-20.
Campbell BCV, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular Therapy for Ischemic Stroke with Perfusion-Imaging Selection. The New England Journal of Medicine. 2015 Mar;372(11):1009-18.
Saver JL, Goyal M, Bonafe A, Diener H-C, Levy EI, Pereira VM, et al. Stent-Retriever Thrombectomy after Intravenous t-PA versus t-PA Alone in Stroke. The New England Journal of Medicine. 2015 Jun;372(24):2285-95.
Jovin TG, Chamorro A, Cobo E, de Miquel MA, Molina CA, Rovira A, et al. Thrombectomy within 8 Hours after Symptom Onset in Ischemic Stroke. The New England Journal of Medicine. 2015 Jun;372(24):2296-306.
©2022 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc
RelatedReports







{kind=link}
