
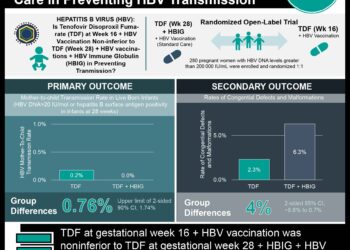
No difference between tenofovir and placebo in reducing perinatal transmission of hepatitis B
1. Hepatitis B e-antigen (HBe-Ag) positive mothers receiving tenofovir daily from 28-weeks gestation to 2 months postpartum did not show significant reductions in HBV transmission rates compared to placebo treated participants.
2. Rates of adverse events, incidences of hepatic flares after treatment discontinuation, or infant growth measures did not differ significantly between the two groups.
Evidence Rating Level: 1 (Excellent)
Study Rundown: Hepatitis B virus (HBV) transmission during the perinatal period is a serious complication during childbirth for HBV positive mothers, as infected infants have a high risk of developing chronic liver disease. Current standard of practice to reduce HBV transmission during childbirth is providing hepatitis B immunoglobulin and hepatitis B vaccinations immediately starting at birth. Recent studies have suggested antiviral therapy during the prenatal period may help reduce the risk of vertical HBV transmission in women with high HBV viral loads. This current analysis compared the efficacy of tenofovir disoproxil fumarate (TDF) versus placebo among mothers who were HBe-Ag positive in reducing the risk of perinatal HBV transmission using a randomized control design. Overall, no significant differences between the two treatment arms were observed, which contrasted with findings from a previous study that reported data on this topic.
Strengths of the current analysis included the use of a placebo-controlled, double-blind design which allowed for comparisons of the two treatment arms. Limitations of this study include inability to generalize these results to broad obstetrical practice, as HBV vaccination regimens differ in Thailand were the study was conducted compared to other countries.
Click to read the study, published in NEJM
Relevant Reading: Tenofovir to prevent Hepatitis B Transmission in Mothers with High Viral Load
In-Depth [randomized controlled trial]: This phase 3, multicenter, randomized, double-blind, placebo-controlled, parallel-group trial randomized 331 women in a 1:1 ratio to receive either TDF (n = 168) or placebo (n = 163). Eligible patients had positive HBsAg and HBeAg tests and non elevated alanine aminotransferase level, and patients with HIV and/or HCV infections were excluded. Treatment with the active drug or placebo was once daily from 28-weeks gestation to 2 months postpartum. Infants also received hepatitis B immunoglobulin at birth, and HBV vaccinations at timed intervals (birth, 1, 2, 4 and 6 months). The primary endpoint of this study was assessment of infants’ HBV infection status at 6 months old. Secondary endpoints included assessment of any maternal or infant adverse events, incidence of maternal hepatic flares, and infant growth at 6 months (weight, height and head circumference).
Results showed that 0 of 147 infants in the TDF group and 3 of 147 in the control group showed signs of HBV infection at their 6-month follow-up (TDF: 95% confidence interval [CI], 0% to 2%; Control: 95% CI, 0% to 6%; p = 0.12). No secondary endpoints were showed significant differences between the groups. One or more adverse events occurred in 41 women in the TDF group versus 44 women in the placebo group (24% vs 27%, respectively; p = 0.62). Common maternal adverse events included increases in alanine aminotransferase levels, and peripartum complications. Adverse event rates among infants in both groups also did not differ significantly (27% in TDF group vs 24% in control group; p = 0.61).
Image: CC/Flickr
©2018 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports








{kind=link}