Posterior circulation stroke patients may benefit from intra-arterial treatment
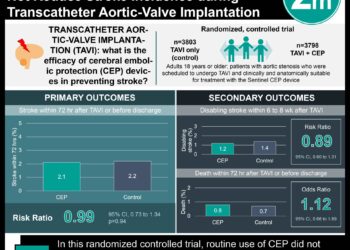
1. In this retrospective case series of 38 patients at University Medical Center Groningen, Netherlands, half of the patients with basilar artery occlusion who underwent intra-arterial treatment had favorable outcomes as defined by a modified Rankin Score of ≥ 3.
2. Intra-arterial treatments in posterior circulation strokes may be beneficial and further randomized studies are warranted.
Evidence Rating Level: 3 (Average)
Study Rundown: Intra-arterial treatment for anterior circulation ischemic stroke has proven benefits in previous studies, however its efficacy in posterior circulation stroke is unclear. This single-center retrospective case series aimed to report the outcomes of patients with basilar artery occlusion (BAO) who received intra-arterial (IA) treatment.
Of the 38 patients with BAO who received IA treatment (thrombolysis, thrombectomy or local thrombolysis administration), 50% had a favorable outcome as defined by a modified Rankin score of ≥ 3 at discharge or follow-up. There was no association between evidence of vascular collaterals and favorable outcome. Two patients had symptomatic intracranial hemorrhage post-procedure. While the study did include consecutive patients and did not have significant exclusion criteria, the retrospective design and the small sample size decrease the generalizability of the results. Rather, this serves as a precursor for a larger, prospective study.
Click to read the study, published today JAMA Neurology
Relevant Reading: Treatment and outcomes of acute basilar artery occlusion in the Basilar Artery International Cooperation Study (BASICS): a prospective registry study
In-Depth [case series]: This retrospective case series was conducted at the University Medical Center Groningen, Netherlands between January 2006 and December 2015. The sample inclusion criteria were all consecutive patients with BAO who underwent IA treatment at this center. Imaging including CT angiography or MRI angiography confirmed BAO. Intra-arterial treatment included thrombolysis, mechanical thrombectomy or a combination of both. Stroke patients were considered eligible for IA treatment depending on individual clinical evaluation. Primary outcomes were disability and dependence in activities of daily living as measured by the modified Rankin score (mRS). A favorable outcome was defined as mRS score of ≥ 3. Secondary outcomes included assessment for vascular collateral flow. Statistical analysis included χ2 or Fisher exact tests. No multivariable regression was performed due to small sample size.
Of the 38 patients who had a BAO and subsequent IA treatment, 27 (71%) had intravenous thrombolysis prior to attempted thrombectomy; mechanical thrombectomy was done in 30 patients (78.9%) and 8 (21%) patients received local urokinase without mechanical thrombectomy. The mean National Institutes of Health Stroke Scale score was 21 (IQR 15-32) and median time to IA treatment was 288 (IQR 216-380) minutes. Favorable outcome (mRS ≥ 3) was observed in 19 (50%) of patients. There was no association between evidence of collateral flow and favorable outcome. Two patients (5%) had a symptomatic intracranial hemorrhage.
Image: CC/Wiki
©2016 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.