No products in the cart.

#VisualAbstract: Moderate hypothermia during venoarterial extracorporeal membrane oxygenation not associated with a decrease in 30-day mortality
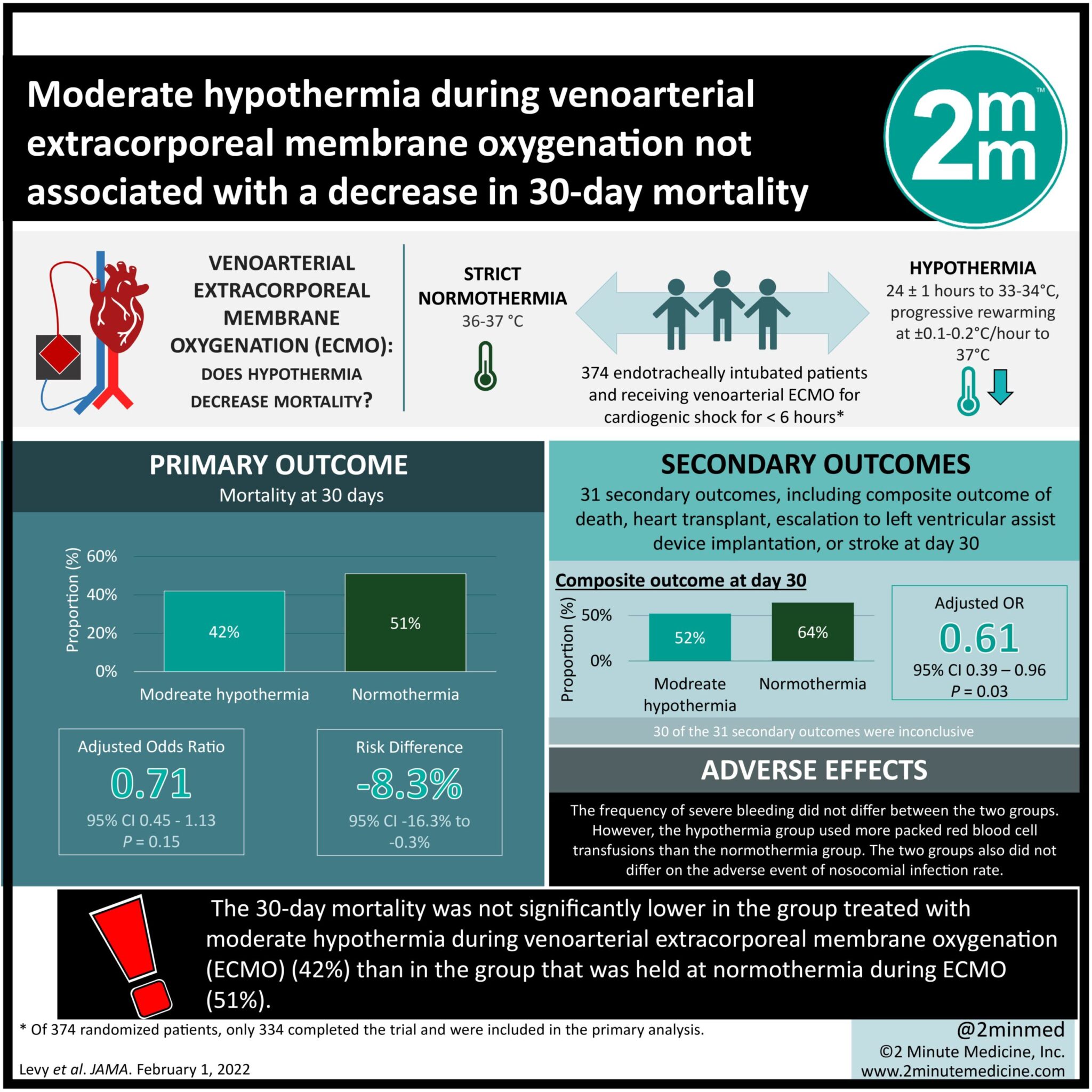
1. The 30-day mortality was not significantly lower in the group treated with moderate hypothermia during venoarterial extracorporeal membrane oxygenation (ECMO) (42%) than in the group that was held at normothermia during ECMO (51%).
2. Adverse events, such as bleeding and nosocomial infections, occurred at a similar rate in the hypothermia and normothermia groups, but the hypothermia group required more red blood cell transfusions.
Evidence Rating Level: 1 (Excellent)
Study Rundown: Venoarterial extracorporeal membrane oxygenation (ECMO) is becoming a more common cardiogenic shock treatment. Patients who require ECMO for refractory cardiogenic shock likely have a severe ischemia-reperfusion injury. Hypothermia may decrease these reperfusion injuries. Thus, the Hypothermia During ECMO (HYPO-ECMO) study attempted to identify if moderate hypothermia (33-34°C) improves the mortality of patients receiving ECMO for cardiogenic shock compared to normothermia (36-37°C). Adult participants in cardiogenic shock were randomized to receive hypothermia or normothermia during ECMO. The hypothermic (n = 168; median Temp = 34.7°C) and normothermic (n = 166; median Temp = 36.4°C) groups were compared, with 30-day mortality being the main outcome. 30-day mortality was 42% for the hypothermic ECMO group and 51% for the normothermic ECMO group, which was not significantly different. However, due to wide confidence intervals, the authors recommend that these results be interpreted with caution. Mortality was reduced in the hypothermia group compared to the normothermia group by 10.4% at day 7, by 6.0% at day 60, but not significantly by day 180. The odds ratio of death, heart transplant, LVAD implantation, or stroke was significantly lower in the hypothermia group compared to the normothermia group by day 30 but was not significantly different by day 60. Hypothermic ECMO patients experienced longer time on a mechanical ventilator, but by day 30 were ventilator-free for the same duration. Adverse events such as bleeding and infection occurred at a similar rate between the two groups, except that the hypothermia group used more packed red blood cell transfusions than the normothermia group. To use therapeutic hypothermia, patients needed to be intubated, sedated, and on mechanical ventilation, which means that these results are not generalizable to all patients that receive ECMO. In addition, the sample size of this trial was small. Consequently, the study included all etiologies of cardiogenic shock, so cannot identify if hypothermia is better for a specific type of cardiopathy. Finally, this study does not measure neurocognitive sequelae, which are clinically important in deciding treatment.
Click to read the study in JAMA
Relevant Reading: Moderate Hypothermia Improves Cardiac and Vascular Function in a Pig Model of Ischemic Cardiogenic Shock Treated With Veno-Arterial ECMO
In-Depth [randomized controlled trial]: Adult patients, stratified by the 20 French intensive care unit cardiac shock care centers involved, were randomized to receive hypothermia-ECMO or normothermia-ECMO. Participants were excluded if they were pregnant, received ECMO after heart or heart and lung transplant, for poisoning, after 45 mins of cardiopulmonary resuscitation, after an out-of-hospital refractory cardiac arrest, received left ventricular assist device implantation, had uncontrolled bleeding, or had irreversible neurological injury. Hypothermia was induced for 24±1 hours, then progressive rewarming at ±0.1-0.2°C/hour to 37°C. Outcomes and adverse events were recorded on days 1 through 7, and days 20, 60, and 180. The main outcome was day 30 mortality. 26% of participants had cardiogenic shock because of acute myocardial infarction and 22% because of decompensated ischemic heart failure. There was a median of 3.0 hours between beginning venoarterial ECMO and initiation of randomization and an additional 30 minutes to the first core body temperature measurement. The moderate hypothermia group (n=168) achieved a median core temperature of 34.7°C compared to the normothermic group (n=166) which had a median core temperature of 36.4°C. 42% of patients receiving hypothermic ECMO, compared to 51% of patients receiving normothermic ECMO, died by day 30, a non-significant difference in odds (adjusted odds ratio [aOR] = 0.71, 95% CI = 0.45−1.13, P = 0.15; risk difference = -8.3%, 95% CI = -16.3%−-0.3%). The risk of mortality was decreased in the hypothermia group compared to the normothermia group at day 7 by 10.4% (95% CI = -16.6%−-4.3%) and at day 60 by 6.0% (95% CI = -16.7%−4.6%), but by day 180 there was no significant difference (aOR = 0.81, 95% CI = 0.51−1.29, P = 0.38; risk difference = -5.5%, 95% CI = -17.5%−6.5%). The combined variable of death, heart transplant, escalation to LVAD implantation, or stroke by day 30 was lower in the hypothermia group compared to the normothermia group (aOR = 0.61, 95% CI = 0.39−0.96, P = 0.03; risk difference = -11.5%, 95% CI = -23.2%−0.2%), which was non-significant by day 60 and 180. The duration of ECMO and the time for patient’s lactate levels to normalize did not differ between the hypothermia and normothermia groups. Hypothermia patients, compared to normothermia patients, had more days without organ failure by day 7. The hypothermia group was on mechanical ventilation for 10 days, compared to 7 days for the normothermia group, but by day 30 the groups did not differ in their number of ventilator-free days. The frequency of severe bleeding did not differ between the two groups. However, the hypothermia group used more packed red blood cell transfusions than the normothermia group. The two groups also did not differ on the adverse event of nosocomial infection rate.
©2022 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports

{kind=link}
