
Catheter-associated UTI prevention program decreases UTI rates in hospital settings
1. A national program deployed in more than 10% of all US hospitals built around disseminating catheter-associated urinary tract infections (UTI) educational materials and collecting UTI data showed a significant reduction in the UTI rates.
2. Catheter associated UTIs were significantly reduced in non-ICU settings, while in ICUs there was no significant change.
Evidence Rating Level: 2 (Good)
Study Rundown: Catheter-associated UTIs are a major source of hospital acquired infection in the US and incidence of these infections has increased in recent years. More than two-thirds of these infections are considered preventable. Following established guidelines regarding technical care of catheters and better assessing sociocultural factors pertinent to patients are considered potential ways to decrease rates of these infections. This study’s goals were to improve safety culture in provider settings on a national level and decrease catheter-associated UTI incidence.
Providers were asked to make daily assessments of catheter necessity for a patient, consider alternative ways of collecting urine, and practice aseptic protocols for catheter insertion and maintenance. The program at each unit lasted 18 months. Catheter-associated UTI rates fell significantly from beginning to end of the study. Catheter use decreased significantly in non-ICU settings but was not significantly changed in ICUs. Furthermore, catheter-associated UTIs decreased significantly in non-ICU settings but not in ICU settings. This study provided a very strong sample size of hospitals (over 600) participating, showing that a widespread preventative program can result in appreciable changes in infection rates, important to providers and patients alike.
Click to read the study, published today in NEJM
Relevant Reading: Preventing catheter-associated urinary tract infection in the United States: a national comparative study
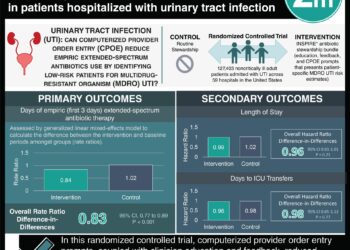
In-Depth [prospective cohort]: Hospital organizations were recruited into the study along with individual hospitals which fell under the organizational structure. The 18-month program occurring at 603 individual hospitals included a total of 1202 sites were recruited into the study, and 926 units were included for study analysis due to completeness of data collection. ICU units made up 40.3% of participating sites, and non-ICU units accounted for 59.7% of sites. The study included a baseline UTI data collection for 3 months, catheter-associated UTI preventative program implementation for 3 months, and follow-up data collection for 12 months. The primary outcome measured was catheter-associated UTI incidence per 1000 catheter-days. From baseline to end of the study, there was a significant decrease in catheter-associated UTIs from 2.40 to 2.05
infections per 1000 catheter-days (incidence rate ratio (RR)=0.86; 95% [CI], 0.76 to 0.96; p=0.009). In non-ICU units, UTIs decreased significantly from 2.28 to 1.54 UTIs per 1000 catheter-days (incidence RR=0.68; 95% [CI], 0.56 to 0.82; p<0.001) while in ICU units they remained unchanged (2.48 to 2.50 UTIs per 1000 catheter-days). Catheter use was significantly
lower in ICUs located in rural areas compared to nonrural areas (incidence RR=0.85; 95% [CI], 0.78 to 0.91; p<0.001). Lastly, catheter use was significantly lower in ICUs in critical-access hospitals than in those in hospitals that were not designated as critical access hospitals (incidence RR=0.81; 95% [CI], 0.67 to 0.98; p=0.03).
Image: PD
©2016 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports








{kind=link}