
Noninvasive DNA assay detects rejection and infection in lung transplant patients [PreClinical]
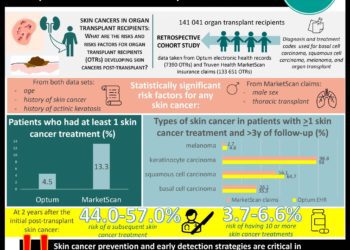
1. High percentages of cell-free donor DNA (cfdDNA) in the plasma of lung transplant recipients correlated with transplant rejection, as measured by transbronchial biopsy scores.
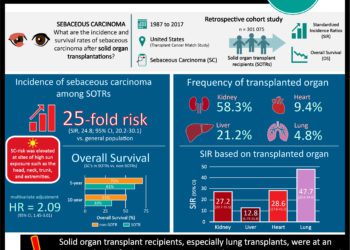
2. High levels of viral cell-free DNA (cfDNA) in the plasma of transplant recipients correlated with clinical reports of cytomegalovirus (CMV) infection and suggested mis- or undiagnosed infections of other pathogens.
Evidence Rating Level: 2 (Good)
Study Rundown: Lung transplants frequently result in complications, including rejection of donor tissue and infection. However, diagnostic tests to determine rejection are limited and invasive, and accurate infection diagnosis relies on identifying the pathogen among many candidates. Here, researchers used cfDNA to simultaneously and noninvasively diagnose both tissue rejection and infection.
Plasma samples were collected from patients over the course of two years following lung transplantation. As expected, levels of cfdDNA circulating in the plasma declined with time following transplantation. Patients diagnosed with moderate-to-severe rejection based on transbronchial biopsy scores, the current gold standard for rejection diagnosis, showed significantly higher plasma levels of cfdDNA as compared to rejection-free patients. Percentages of cfdDNA were also significantly higher in patients showing clinical signs of rejection, chronic lung allograft dysfunction (CLAD), or antibody-mediated rejection (AMR).
Non-human cfDNA in patient plasma was used for infection diagnosis. High levels of cfDNA from CMV, a pathogen of particular concern in post-transplant patients, were a reliable indicator of CMV infection. The authors also demonstrated that a number of samples contained elevated cfDNA from other pathogens which were not otherwise screened for, suggesting that many infections escape diagnosis or are misdiagnosed.
One barrier to establishing the efficacy of this new approach is that rejection was established based on transbronchial biopsy scores, which are highly observer-dependent. Additionally, infection diagnosis may be limited to pathogens which are not usually found in the body and therefore have a low background cfDNA percentage. These concerns notwithstanding, this study presents a noninvasive, extensive and inexpensive way to diagnose both rejection and infection in lung transplant recipients.
Click to read the study in PNAS
Relevant Reading: Pulmonary Complications of Lung Transplantation
In-Depth [prospective cohort]: 51 patients were recruited for the study, with 44 undergoing bilateral lung transplants and 7 undergoing single lung transplants. 398 plasma samples in total were collected from these patients over the course of two years following transplantation.
Initially, the authors showed that cfdDNA declined from about 26% in patient plasma immediately following transplantation to under 1% within several months. Patients with moderate-to-severe rejection as diagnosed by transbronchial biopsy had higher cfdDNA levels than rejection-free patients (p=5e-04, n=7-85 per group). A receiver-operating characteristic (ROC) analysis, which plots the true positive rate against the false positive rate, yielded an area under the curve (AUC) of 0.9 for the ability of cfdDNA level to predict moderate-to-severe rejection. Levels of cfdDNA were also higher in plasma from patients showing clinical signs of rejection (p=6e-04, n=53-226), CLAD (p=1e-04, n=19-246) and AMR (p=0.0437, n=9-225), as well as those treated for rejection (p=5e-04, n=58-222).
Analyzing non-human cfDNA for infection diagnosis showed that elevated CMV cfDNA levels correlated with samples testing positive for CMV infection (p=7e-09), with an AUC of 0.91. The authors also found elevated cfDNA levels of several other pathogens which are less commonly screened for, including adenovirus and polyomavirus, in approximately the same number of samples as those with elevated CMV cfDNA levels. They concluded by demonstrating several cases where a patient not tested for a particular pathogen showed similar cfDNA plasma levels as those in a patient who tested positive for the same pathogen, suggesting that their approach could more extensively diagnose infectious sources than current methods and ultimately lead to proper treatment.
Image: PD
©2015 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports



![Adverse pregnancy outcomes associated with thrombophilias [Classics Series]](https://www.2minutemedicine.com/wp-content/uploads/2015/07/Classics-2-Minute-Medicine-e1436017941513-75x75.png)

{kind=link}
