Patient Basics: Prostate Cancer
Originally published by Harvard Health.
What Is It?
Prostate cancer results from the uncontrolled growth of abnormal cells in the prostate gland. This gland produces part of the fluid in semen. It is located below the bladder and in front of the rectum, near the base of the penis.
Prostate cancer is one of the most commonly diagnosed cancers in American men. Many other men have the disease, but have not been diagnosed. This is because prostate cancer has few symptoms early on.
Prostate cancer is common, but it is not always dangerous. This is because it usually grows very slowly. It affects older men; the average age at diagnosis is 70. And it’s usually diagnosed before it causes any symptoms. Also, these men often have other illnesses which may be more important to treat than a cancer that doesn’t cause symptoms.
When cells in the prostate become cancerous (malignant), they clump together, forming small “islands” of cancer in the prostate. In many cases, it takes years, even decades, for this localized cancer to spread beyond the prostate. And many of these cancers may never spread.
Researchers do not know the exact cause of prostate cancer. But they have identified several factors that raise a man’s risk of the disease. These include:
- Age. Autopsy studies of men who died of other causes have found that about three-quarters or more of them have some degree of prostate cancer by age 80. These men didn’t know they had prostate cancer.
- Race. African American men are more likely to get prostate cancer than other men—and to be diagnosed when the cancer is at a more advanced stage. They are also more than twice as likely to die of the disease as white men and about five times more likely to die of it than Asian Americans.
- Family history. If a man’s father or brother has been diagnosed with prostate cancer, his cancer risk is two to three times higher than a man who doesn’t have family members with the disease. Researchers have identified several genetic defects that may be more common in men who develop prostate cancer. But overall, most experts say that inherited defects cause a relatively small number of cancers. Recent research also links a higher risk of developing prostate cancer in families whose female members are at higher than average risk to develop breast cancer. A common genetic abnormality may be responsible for an increased risk to both prostate and breast cancer.
- Lifestyle. Men who eat a lot of red meat or high-fat dairy products seem to have a higher risk of prostate cancer. There is little evidence that being overweight increases the risk of prostate cancer. However, obese men are more likely to die of the disease than men at a healthy weight.
Symptoms
In its early stages, prostate cancer rarely causes symptoms. In fact, most men diagnosed with prostate cancer have no symptoms. Doctors suspect prostate cancer if a blood test shows high levels of prostate-specific antigen (PSA). However, if the cancer spreads to the bladder or presses on the urethra, the tube that carries urine out of the body, it can cause:
- a weak urine stream
- a need to urinate often
- an intense need to urinate
- an inability to urinate
- pain or burning when you urinate
- blood in your urine or semen
- erections that are less firm
- a drop in the amount of semen ejaculated
- pain or stiffness in your lower back, hips, or upper thighs.
If prostate cancer spreads to the lymph nodes, bones, or other organs, it can cause
- bone pain
- weight loss
- anemia (a lack of red blood cells)
- shortness of breath
- swelling in the scrotum, penis, legs, and feet
- fatigue.
Diagnosis
Your doctor will ask about your symptoms, your medical history, and whether prostate cancer runs in your family. Your doctor will want to know whether you have ever been diagnosed with an inflamed or enlarged prostate. These conditions are not cancerous. However, the symptoms of these conditions can be the same as symptoms of prostate cancer.
Your doctor will examine you and do a digital rectal exam (DRE) to feel the prostate gland. During a DRE, the doctor inserts a gloved, lubricated finger into the rectum. The doctor can feel part of the prostate through the rectal wall. Swelling, lumps, firm spots, or enlargement may indicate prostate cancer.
Most cases of prostate cancer are detected by screening for the disease with a PSA test. PSA is a protein made by the prostate that can be detected in blood. Prostate cancer can cause higher amounts of PSA to leak out of the prostate into the blood. Tell your doctor if you take any medications to treat an enlarged prostate. Certain prostate medications, such as finasteride (Proscar) and dutasteride (Avodart), can affect PSA test results.
Although doctors use the PSA test to detect prostate cancer, it does not give a definitive diagnosis. That’s because other conditions, such as an enlarged prostate, can raise PSA levels. In fact, most men with a mildly elevated PSA do not have prostate cancer. Also, some men with a normal PSA actually do have cancer.
Because an elevated PSA level may prompt you to seek treatment, which can cause urinary and sexual side effects, many doctors and organizations don’t recommend routine PSA screening. Instead, they suggest that men age 50 and older talk with their doctors about the risks and benefits of screening. African American men should talk with their doctors about PSA screening beginning at age 40.
Even though PSA screening is the most common way prostate cancers are detected, the test very often finds cancers that do not need to be treated. In fact, some medical organizations now recommend not having the test performed on a routine basis.
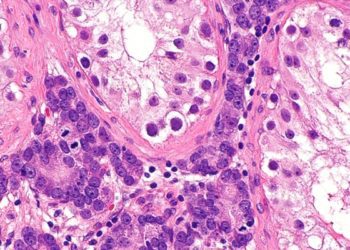
If your PSA level is high, or if your DRE shows a possible problem, your doctor may order more tests, such as a prostate biopsy. In this procedure, a needle is used to remove small pieces of tissue from the top, middle, and bottom parts of the prostate. Your doctor also may want to take tissue samples from any areas that felt abnormal during the DRE. A specialist called a pathologist then checks the tissue samples for cancer under a microscope.
If your biopsy shows prostate cancer, the pathologist will assign a Gleason grade to the two most common cells types in your tumor. The sum of the two grades is the Gleason score. The Gleason score describes how abnormal the cancer cells look compared to normal prostate cells. The score provides a rough estimate of how fast the cancer is growing. A Gleason score of
- 2 to 4 means low-grade, nonaggressive cancer
- 5 to 7 means intermediate-grade cancer
- 8 to 10 (ten is the highest score) means high-grade, aggressive cancer.
A doctor will also assign a “stage” to your cancer. The stage describes the extent of the tumor and whether it has spread. Doctors use the Gleason score and stage to plan treatment.
Expected Duration
Once prostate cancer develops, it usually grows slowly over many years. In a small number of men, prostate cancer grows and spreads quickly. Almost all prostate cancer will respond to some type of treatment. In some cases, prostate cancer might not need treatment right away, if at all. Doctors have developed criteria to determine which cancers need treatment and which ones can be watched. If a watched tumor worsens, it can be treated.
Prevention
Although the evidence is mixed, men who eat a low-fat diet rich in fruits and vegetables may reduce their risk of prostate cancer. Older studies suggested that eating tomatoes, which contain the antioxidant lycopene, might reduce risk. Recent studies have questioned lycopene’s value.
Some medications have been tested to see if they prevent prostate cancer. These include finasteride and dutasteride, drugs normally prescribed for benign prostate enlargement. One study showed that men who took finasteride reduced their prostate cancer risk by 25 percent. But it also found that the risk of aggressive cancer went up in some men. Later studies found that the drug doesn’t increase aggressive tumors. Given the contradictory findings, experts don’t agree about whether to offer finasteride to men with a higher risk of prostate cancer than normal.
Treatment
Prostate cancer can be treated several ways. You and your doctor should weigh medical and lifestyle issues before choosing a treatment. These include
- the extent of your cancer
- the chance that your cancer will grow and spread rapidly
- your age and how long you might live
- any health conditions that would make surgery or other treatments riskier
- your willingness to risk side effects.
If your cancer is confined to the prostate gland, you have several options.
Watchful waiting. With this approach, you don’t have treatment unless you begin to have symptoms. Your doctor will monitor your cancer with DREs and PSA tests from time to time. This strategy is a good option for elderly men who are too ill for radiation or surgery, or who are likely to die from another medical condition relatively soon.
Active surveillance. Men whose prostate cancer doesn’t need treatment right away may opt for active surveillance. If you choose this approach, you will be followed more closely than with watchful waiting. Every three to six months, you will have a PSA test and a physical exam. You may also have a biopsy every year or two. If any of these show increased disease activity, you can start treatment.
Radiation therapy. This treatment uses radiation to destroy cancer cells. Doctors can deliver radiation in two ways. The first method involves directing radiation into the body from outside the body. This is called external beam radiation therapy. Several types exist, but the goal with each is to precisely target the prostate and spare healthy tissue.
The second method involves putting small radioactive pellets, or seeds, into the prostate gland. Your doctor may call this brachytherapy, seed implantation, or interstitial radiation therapy. In most cases, the seeds are left in place permanently.
Your doctor may prescribe hormone therapy to boost the effectiveness of radiation therapy. He or she may also prescribe hormone therapy to shrink the prostate before brachytherapy.
Side effects of radiation therapy can include
- erectile dysfunction (the inability to have an erection)
- diarrhea
- rectal bleeding and pain
- urinary incontinence (the inability to hold urine)
- blood in the urine
- fatigue.
Surgery. During a radical prostatectomy, the doctor will remove your prostate gland and seminal vesicles. (Seminal vesicles are glands that release fluid that becomes part of semen.) The doctor may also remove the nearby pelvic lymph nodes. During surgery, the doctor will try to do as little damage to nearby nerves as possible. This can reduce side effects such as erectile dysfunction and incontinence.
The doctor may use any of several techniques. For example, he or she may remove the prostate through an incision in the abdomen. Or he or she may operate laparoscopically, removing the prostate and other tissues through several tiny incisions. This is often done with the aid of a robot machine to help visualize and remove the prostate. This is called RALP (robotically assisted laparoscopic prostatectomy). Possible complications of prostate surgery include
- erectile dysfunction
- urinary incontinence
- bowel problems
- infection.
The chances of dying during or right after surgery are very low.
Cryoablation. This treatment, also called cryotherapy, kills cancer cells by freezing and then thawing them. It isn’t offered at many hospitals, so finding an expert to perform the procedure in your area may be difficult. Additional research is needed to determine the long-term effects of cryoablation.
High intensity focused ultrasound. This treatment destroys prostate cancer with high energy sound waves that heat cells to high temperatures. It is not currently an approved treatment for prostate cancer. Ongoing studies should help doctors determine if this procedure is safe and effective.
If your prostate cancer has grown through the prostate capsule but has not spread (metastasized) to other organs, watchful waiting or radiation therapy (with or without hormone therapy) are usually recommended.
If the cancer has spread to other organs, doctors usually prescribe hormone therapy, also called androgen-deprivation therapy. Androgens are male sex hormones, such as testosterone. Androgens can fuel prostate cancer. Hormone therapy reduces testosterone by preventing the testicles from producing it. Another approach is to surgically remove the testicles. However, few men opt for this procedure.
Side effects of hormone therapy include
- erectile dysfunction
- breast enlargement
- decreased sex drive
- hot flashes
- weight gain
- nausea and diarrhea
- a drop in bone density and muscle mass
- changes in liver function.
If prostate cancer has already spread to other organs at the time of diagnosis, doctors may either start hormone therapy alone or a combination of both hormone therapy and chemotherapy.
When To Call a Professional
Call your doctor right away if you notice blood in your urine or semen, or if urination is painful, uncomfortable, or abnormal in any way.
If you are age 50 or older, ask your doctor about the pros and cons of prostate cancer screening. Some experts believe screening with PSA tests and DREs saves lives because cancer can be detected early. Others say that screening causes more harm than good. That’s because some men will suffer side effects from treatment they may not have needed. Your doctor can help you decide whether screening makes sense for you.
If you decide to get screened, your doctor probably will do a prostate exam and check your PSA level every one to two years, starting at age 50. If prostate cancer runs in your family, or if you are African American, screening may start at age 40.
Prognosis
The prognosis usually is excellent. Nearly all men diagnosed with localized cancer survive at least five years. More than three-quarters of all men diagnosed with the disease live at least 15 years. In fact, many more men die of other causes while they have prostate cancer than die as a result of the cancer.
Additional Information
National Cancer Institute (NCI)
U.S. National Institutes of Health
Public Inquiries Office
6116 Executive Blvd.
Room 3036A
Bethesda, MD 20892-8322
http://www.nci.nih.gov/
American Cancer Society (ACS)
1599 Clifton Road, NE
Atlanta, GA 30329-4251
http://www.cancer.org/
American Urological Association
1000 Corporate Blvd.
Linthicum, MD 21090
http://www.urologyhealth.org/
RelatedReports

![2 Minute Medicine: Pharma Roundup: Price Hikes, Breakthrough Approvals, Legal Showdowns, Biotech Expansion, and Europe’s Pricing Debate [May 12nd, 2025]](https://www.2minutemedicine.com/wp-content/uploads/2025/05/ChatGPT-Image-May-12-2025-at-10_22_23-AM-350x250.png)