



{kind=link}


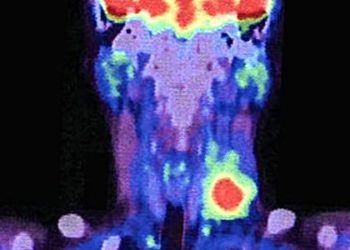
PET/MRI is viable for tracking small lung nodules in cancer patients
1. Positron emission tomography and magnetic resonance imaging (PET/MRI) was not as sensitive as PET and computed tomography (PET/CT) for the detection of small pulmonary nodules.
2. The majority of nodules that were missed when using PET/MRI either resolved or remained stable over time, suggestive of benignity, and did not affect the clinical management of the patient.
Evidence Rating: 4 (Below-Average)
Study Rundown: Positron emission tomography combined with computed tomography (PET/CT) has served as the gold standard for the staging and restaging of a variety of cancers. However, PET combined with magnetic resonance imaging (PET/MRI) allows for greater contrast resolution of MR without radiation exposure and the metabolic information of PET to help determine the tumor burden in patients, but concerns exist regarding the ability of MRI to detect lung nodules that are less than 1cm in diameter, which is below the resolution of PET imaging. MRI is notoriously limited in its ability to image the lung parenchyma due to low proton density, air-tissue interfaces and motion degradation, however newer fast-imaging sequences have overcome some of these issues. This study evaluated patients with full body PET/MRI with known primary malignancy who were already undergoing PET/CT for staging purposes, specifically looking at small pulmonary nodules. There were 43 patients who had 89 non-FDG avid small lung nodules detected on PET/CT that were not detected on PET/MRI. Only 84 of the 89 nodules had subsequent imaging with PET/CT or chest CT, while the last five had remote imaging available for evaluation. Of these 84 nodules, three nodules (3%) in one patient progressed, 10 (12%) nodules had some or complete resolution, and 71 (85%) remained stable. The five nodules lost to follow up were stable at 21 months. The mean size of the 89 small lung nodules was 0.4±0.19 cm (range 0.2-1 cm). Overall, 97% of small nodules missed on PET/MRI were stable or resolved on follow-up imaging. This study establishes that while PET/MRI may not be as sensitive as PET/CT, the majority of missed nodules were benign, and therefore this imaging modality may represent a viable strategy for follow up in oncology patients, particularly for those in whom radiation exposure must be limited. The primary limitation of this study was the relatively small size and the heterogeneity of patient demographics and primary malignancy types, which may limit overall generalizability. Future studies should determine if PET/MRI is capable of detecting which of these nodules are more likely to progress, and how confidently PET/MRI can identify nodules that will remain stable.
Click to read the study in Journal of Magnetic Resonance Imaging
Relevant reading: Pulmonary lesion assessment: comparison of whole-body hybrid MR/PET and PET/CT imaging—pilot study
In-Depth [case series]: A total of 208 patients (66% female, mean age 73 years) with a known primary malignancy were enrolled over a 10 month period to undergo whole body PET/MRI immediately after undergoing PET/CT. Patients received oral and intravenous contrast agents, in addition to (18F) fluorodeoxyglucose (FDG), and underwent MR examination with a 3 tesla magnet. There was a mean of 174.8 minute delay from tracer injection to initiation of PET/MR scanning. MR sequences used included T1-weighted gradient echo imaging with radial stack-of-stars trajectory (STAR VIBE), diffusion weighted imaging with a spin echo single-shot echo-planar imaging sequence. Image interpretation for PET/CT was performed by 2 independent readers (radiologist and nuclear medicine physician) and compared to the results of PET/CT imaging, which were used as the reference standard after a delay of 2 weeks prior to the evaluation of the PET/MR images. There were 45 patients who had non-FDG lung nodules that measured 1cm or less that were detected by PET/CT but not PT/MRI, but two were excluded due to loss of follow up. Of the 71 nodules that remained stable, 62/71 were also stable since older studies over a period of 11-78 months (mean 36.6 months). In a review of the electronic charts, patient management did not change in lieu of these missed nodules. Interreader agreement kappa values were 0.375 for PET/CT (fair) and 0.68 for PET/MR (substantial).
Image: PD
©2015 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
