




{kind=link}


2 Minute Medicine Rewind March 4, 2019
Cervical artery dissection is a common cause of ischemic stroke in young patients. Whether antiplatelet (AP) therapy or anticoagulation (AC) therapy is more effective at preventing recurrent stroke after dissection is unknown. In 2015, data from the Cervical Artery Dissection in Stroke Study (CADISS) trial showed no difference in event rates in patients treated with AC or AP at the primary endpoint of 3 months. In this study, the authors report the 1-year follow-up data from CADISS. In this randomized controlled trial, 250 patients with extracranial carotid and vertebral artery dissections with symptom onset in the prior 7 days were assigned to receive either AP or AC therapy for at least 3 months to compare the impact on the incidence of ipsilateral stroke and death. AP therapy consisted of aspirin, clopidogrel, dipyridamole, or a dual combination. For AC therapy, the recommended regimen was heparin (either unfractionated heparin or low-molecular-weight heparin) followed by warfarin, aiming for an international normalized ratio (INR) in the range of 2 to 3. At baseline, 118 patients had carotid artery dissection, and 132 had vertebral artery dissection. The most common presenting symptom was cerebral ischemia (224 patients). In the AP arm, 22.2% of patients received aspirin alone, 22.2% received clopidogrel alone, 0.8% received dipyridamole alone, 27.8% received aspirin and clopidogrel, and 15.9% received aspirin and dipyridamole. In the AC arm, 90.3% of patients received heparin and warfarin, and 9.7% received warfarin alone. Based on an intention-to-treat analysis, researchers found that at 12 months after randomization, there was no significant difference in the incidence of ipsilateral stroke, (OR 0.56, 95% CI 0.10 to 3.21). There were no deaths in the AC group and one death in the AP group, owing to a fatal recurrent stroke between 3 and 12 months in a patient who had a first recurrent stroke within the first 3 months. There was one major bleed in a patient in the AC group. Overall, results from this study show that the risk of recurrent stroke or death after cervical artery dissection is low, and that there is no difference in efficacy between anticoagulation and antiplatelet therapy in reducing this risk.
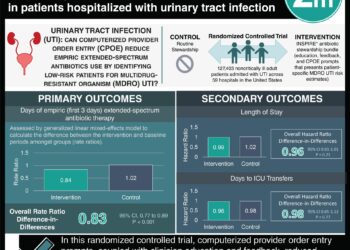
Urinary tract infection (UTI) is the most common bacterial infection in elderly patients, and the spectrum of illness ranges from mild and self-limiting to severe urosepsis. More evidence is needed to determine the ideal initial management of UTI in the primary care setting. In this retrospective cohort study, 312,896 UTI episodes from 157,264 unique patients age 65 years or older were studied to assess the impact of antibiotic prescribing practices on bloodstream infections, hospital admission, and all-cause mortality within 60 days after the index UTI diagnosis. The mean age of the study cohort was 76.7 years, and at the time of initial UTI diagnosis, 78.8% of participants were women, 40.3% originated from the south of England, and 28.9% were from the most deprived areas. Immediate antibiotic prescribing was defined as prescription of an antibiotic during the first UTI visit or on the same day, and deferred antibiotic prescribing was defined as prescription of an antibiotic within 7 days of the first UTI visit. Among all UTI episodes, 7.2% did not have a record of antibiotics being prescribed, and in 6.2%, there was deferred antibiotic prescribing. After adjusting for covariates, researchers found that the rate of bloodstream infection within 60 days was significantly higher among patients who were not prescribed an antibiotic compared with those who received immediate antibiotic treatment (2.9% vs. 0.2%, OR 8.08, 95% CI 7.12 to 9.16, p<0.001), and was also higher among patients who received a deferred antibiotic prescription (2.2% vs. 0.2%, OR 7.12, 95% CI 6.22 to 8.14, p<0.001). Additionally, the rate of hospital admissions was significantly higher in cases that did not receive antibiotics (27.0%) or received deferred antibiotics (26.8%) compared to those that received immediate antibiotics (14.8%, p<0.001). Finally, the risk of all-cause mortality was significantly higher in cases with no antibiotics and with deferred antibiotics than in those with immediate antibiotics during the 60-day follow-up period (HR 2.18, 95% CI 2.04 to 2.33 and HR 1.16, 95% CI 1.06 to 1.27, respectively). Overall, this study supports immediate initiation of antibiotics in elderly patients with a diagnosis of UTI.
Cutaneous squamous cell carcinoma of the head and neck (cSCC-HN) generally has a favorable prognosis, however, there is a subset of patients who experience a more aggressive clinical course. A previous study showed that patients with aggressive cSCC-HN and who are chronically immunosuppressed have a lower rate of progression-free survival following surgery and postoperative radiotherapy (RT) as compared to immunocompetent patients. However, outcomes of cSCC-HN patients following disease recurrence after surgery and postoperative RT are unknown. In this retrospective cohort study, 205 patients who underwent surgical resection and postoperative RT for primary or recurrent stage I to IV (non-metastatic) cSCC-HN were studied to assess overall survival. Of the original cohort, 55.6% were immunosuppressed, defined as patients who received a diagnosis of chronic hematologic malignant neoplasm, HIV/ AIDs, or were treated with immunosuppressive therapy for organ transplantation at least 6 months prior to diagnosis of cSCC-HN. Overall, 72 patients (63 men and 9 women, median age 71 years) developed disease recurrence. The median time to any disease recurrence after completing postoperative RT was 10.1 months (range 1.4 months to 57.4 months) in immunocompetent patients and 9.1 months (range 1.0 months to 77.4 months) in immunosuppressed patients. Researchers found that, after any recurrence, the 1-year overall survival was 43.2% (95% CI 30.9% to 55.4%) and median survival was 8.4 months for the entire cohort. There was no statistically significant difference in median survival between immunocompetent and immunosuppressed patients (12.9 months vs. 8.0 months, p=0.90). Of the 45 patients for whom data on salvage treatment was available, patients who were not amenable to surgical salvage had significantly lower median cumulative incidence of survival compared with those who were amenable to surgical salvage (4.7 months vs. 26.1 months, p=0.01). Survival was not significantly different between immunocompetent and immunosuppressed patients with unsalvageable disease (5.0 months vs. 3.9 months, p=0.09). In summary, this study illustrates the poor overall survival of cSCC-HN patients who experience disease recurrence, regardless of immune status. Survival rates are especially low for patients who were not amenable to surgical salvage.
Antibiotic resistance is a growing challenge across the globe. As such, there have been increasing efforts towards reducing unnecessary or inappropriate antibiotic prescribing of antibiotics. There is limited evidence regarding the contribution of excessive antibiotic treatment duration to antibiotic overuse in the primary care setting. In this cross-sectional study, 931,015 consultations for 13 different indications that led to antibiotic prescriptions were included in the analysis to study the percentage of antibiotic prescriptions with a duration exceeding the guideline recommendation, and the total number of days beyond the recommended duration for each indication. Data were obtained from The Health Improvement Network (THIN), a primary care database representative of the general UK population, from 2013 to 2015. The 13 indications were: acute sinusitis, acute sore throat, acute cough and bronchitis, pneumonia, acute exacerbation of chronic obstructive pulmonary disease (COPD), acute otitis media, acute cystitis, acute prostatitis, pyelonephritis, cellulitis, impetigo, scarlet fever, and gastroenteritis. The Public Health England (PHE) provided guidelines for antibiotic regimens. The most common indications for antibiotics were acute cough and bronchitis (41.6%), acute sore throat (25.7%), acute otitis media (8.9%), and acute sinusitis (8.2%). Researchers found that upper respiratory tract infections and acute cough and bronchitis accounted for more than two-thirds of total prescriptions, and 80% or more of these treatment courses exceeded guideline recommendations (acute cough and bronchitis: 85.6%; acute sore throat (5-day recommended duration): 83.8%; acute COPD exacerbation: 89.0%). A notable exception was seen in the management of acute sinusitis, for which only 9.6% of prescriptions were longer than the guideline recommendation. For all conditions grouped together, antibiotic regimens were prescribed for about 1.3 million days beyond the durations recommended by guidelines. In summary, this study underscores that for some of the most common infections in primary care, antibiotics are often prescribed for a longer duration than is recommended by current guidelines.
The use of digital breast tomosynthesis (DBT) has been associated with increases in specificity and breast cancer detection compared with digital mammography (DM) alone. However, most published studies employed data from first- or prevalent-round screening rather than incident-round screening. In addition, few studies contained data such as age, breast density, and cancer molecular subtypes. Therefore, the role of DBT in breast cancer screening across all ages, breast density groups, and tumor subtypes remains unclear. In this prospective cohort study, 96,269 women age 40 to 74 years who underwent screening examinations using DM and DBT were evaluated to study the primary outcomes of recall rate, cancer detection rate, positive predictive value, biopsy rate, and distribution of invasive cancer subtypes, as well as their associations with DM and DBT. Of 180,340 breast cancer screening examinations performed, 71.7% used DM and 28.3% used DBT. DBT was slightly more common among younger women, women with dense breasts, and those undergoing their first screening. Researchers found that the recall rate was lower for DBT compared with DM (8.7% vs. 11.2% respectively, OR 0.64, 95% CI 0.57 to 0.72, p<0.001), and that the breast cancer detection rate was higher with DBT than with DM for all age groups (OR 1.41, 95% CI 1.05 to 1.89, p=0.02). Overall breast cancer rates were higher with DBT than with DM (OR 1.47, 95% CI 1.12 to 1.94, p=0.01), with the greatest association among women aged 40 to 49 years (OR 1.70, 95% CI 1.04 to 2.77, p=0.03). For these younger women, breast cancers detected by DBT were less often classified as advanced cancers compared with cancers detected through DM, however, this difference was not statistically significant (25% vs. 40.4%, p=0.17). After adjusting for confounding factors, screening examinations with DBT were associated with higher specificity (OR 1.46 95% CI 1.30 to 165, p<0.001). Overall, results from this study suggest that DBT may have a higher specificity for breast cancer than DM, and supports the use of DBT screening in younger women.
Image: PD
©2019 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
