


{kind=link}


Mechanical aortic valve replacement linked with increased early mortality
1. When compared with bioprosthetic aortic valve replacements (AVR), mechanical AVRs were associated with increased mortality on the date of surgery and in early days after the operation amongst older Americans.
2. This difference in mortality was not present between the two forms of AVR 30 days after the operation.
Evidence Rating Level: 2 (Good)
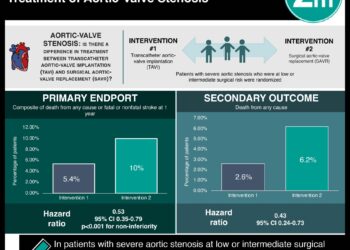
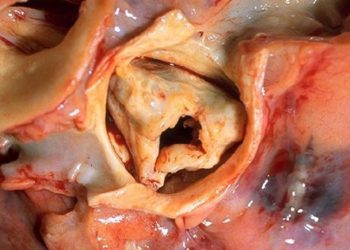
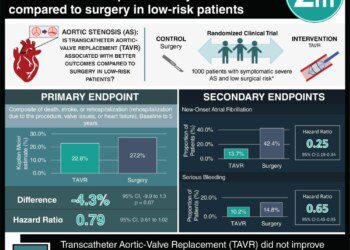
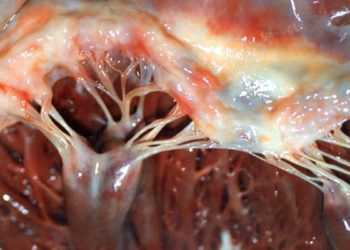
Study Rundown: Symptomatic aortic stenosis is a major reason that patients undergo valve replacement surgery. Currently, there are two options: mechanical valves, which are very durable but require lifelong anticoagulation, and bioprosthetic valves, which do not require long term anticoagulation but are not as durable. While the American Heart Association recommends bioprosthetic valves in older Americans, there has not been any evidence to suggest that one is superior to another in terms of early mortality. This cohort study was designed to help answer that question. The results of this study suggest that bioprosthetic aortic valves were associated with decreased mortality during and immediately after the surgery compared to mechanical aortic valves. However, this difference was not observed after the first 30 days of the operation.
The major strength of this observational study is the large number of patients included in the cohort. Since only Medicare patients were included in the study, the results are only generalizable to the older adult population, not to the young patients undergoing AVR. Furthermore, there were major confounding factors present, such as concurrent coronary artery bypass graft surgeries, demographic differences, and the use of anticoagulants for comorbidities, which make the interpretation of the results somewhat difficult.
Click to read the study, published today in JAMA Internal Medicine
Relevant Reading: Valve type and long-term outcomes after aortic valve replacement in older patients
In-Depth [retrospective cohort]: The study cohort consisted of Medicare beneficiaries of age 65 yrs or older undergoing an aortic valve replacement between July 1, 2006 and December 31, 2011. The primary outcome was all-cause mortality after AVR. Since there were significant differences between the groups of patients receiving the two different aortic valves and the locations in which these were performed, the investigators use mixed-effect modeling to develop a logistic regression to help control for the covariables.
In this modeling, the mechanical valves, when compared with the bioprosthetic valves, were associated with a greater risk of death on the date of the surgery (adjusted OR, 1.61; 95% CI, 1.27-2.04; P<0.001). The same was true for mortality in the first 30 days after the surgery (adjusted OR 1.18; 95% CI, 1.09-1.28; P<0.001). Operative mortality was also greater in patients undergoing the mechanical AVR (adjusted OR, 1.21; 95% CI, 1.13-1.30; P<0.001). There was no significant difference in morality between the two different types of AVR after the first 30 days of the operation (adjusted OR, 1.04; 95% CI, 0.93-1.17; P=0.50).
More from this author: Proton pump inhibitor boluses as effective as infusions in ulcer bleeds, Intensity of medical residency may affect future practice style, Coronary angiography in asymptomatic patients may lead to inappropriate percutaneous interventions, Blood clot prophylaxis medicine inpatient may be unnecessary, Chest pain may be better than EKG, echo for predicting coronary artery disease prognosis
Image: PD
©2012-2014 2minutemedicine.com. All rights reserved. No works may be reproduced without expressed written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors, editors, staff or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT.
RelatedReports
