
Antibiotic prophylaxis not associated with UTI prevention in children [Pediatrics Classics Series]
Image: PD
1. Among children recruited following febrile urinary tract infection (UTI) and randomized to receive either antibiotics or no medication, no significant difference in UTI recurrence was noted between groups.
2. Male children and those with grade III vesicoureteral reflex had significant reductions in subsequent UTIs if treated with prophylactic antibiotics.
Original Date of Publication: February 2008
Study Rundown: In the years leading up to this study, physicians often prescribed antibiotic prophylaxis to children at perceived increased risk for repeat urinary tract infections (UTIs), particularly those with vesicoureteral reflux (VUR). As multiple UTIs have been linked to renal scarring and nephropathy, preventing recurrence is highly important. However, with some studies indicating that antibiotics might be ineffective at preventing UTIs, this study took a prospective, randomized approach to investigate the effectiveness of prophylactic antibiotics in pediatric patients with mild VUR. This randomized, multi-center prospective study found no significant difference in repeat UTI among children with mild VUR who did or did not receive prophylactic antibiotics. A significant increase in risk for a second UTI was seen in those with grade III mild VUR and significant reduction in repeat UTI with treatment was observed in males. This study was limited in its lack of a blinded approach and placebo for control group “treatment” along with the use of potentially contaminated urine specimens from urine bags and uncircumcised males. It also lacked assessment for antibiotic compliance. This study raised questions regarding the necessity to prescribe prophylaxis for all young children following first febrile UTI and the need to obtain voiding cystourethrogram (VCUG) for all children in order to determine VUR presence. As unnecessary treatment is linked to potential adverse drug effects coupled with organism resistance, careful consideration should be taken in prescribing antimicrobial medication. In the time since this study’s publication, many more research projects have investigated UTI risk in children. The most recent American Academy of Pediatrics (AAP) practice guidelines for UTI management in young children are below and recommend renal and bladder ultrasound prior to VCUG and VCUG only if abnormal findings are found on ultrasound. Use of prophylactic antibiotics following initial UTI is not recommended, but potential further investigation of prophylaxis value among males with higher grade VUR is proposed.
Click to read the study in The Journal of Urology
Click to read the current AAP practice guidelines
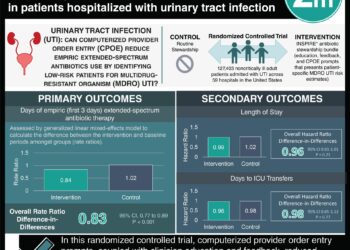
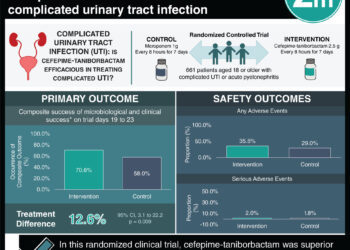
In-Depth [randomized, multi-center prospective study]: From June 2001 to December 2004, 225 patients (31% male) 1 month to 3 years of age with low grade VUR diagnosed on voiding cystourethrogram following febrile UTI were recruited from 17 French pediatric facilities. VUR was graded by severity into grade I, grade II, or grade III VUR and grouped by laterality (unilateral or bilateral). Participants were randomized to receive either trimethoprim (2 mg/kg)/sulfamethoxazole (10 mg/kg), also known today as Bactrim (n = 103, 46%), or no medication (n = 122, 54%). Follow-up renal ultrasound (US) was performed 9 and, 18 months after study initiation, both US and VCUG were completed. UTI was a study endpoint with children who experienced a UTI, defined as > 105 bacteria per mL of urine, excluded from the study and the UTI noted.
Following study initiation, 50 children, 18 in the treatment group (17%) and 32 in the control group (26%), experienced a second UTI. There was no significant difference between the two groups in terms of UTI rates (p = 0.15). There was also no significant difference between groups regarding the diagnosis of febrile UTI (13 or 13% in treatment group v. 19 or 16% of the control group, p = 0.52). The majority of UTI recurrence occurred in females (78%). Males who received prophylactic treatments had significantly less UTI than those who went untreated (39, 57% in untreated v. 30, 43% in treated, p < 0.05). This effect was not seen among females. No significant differences were seen between groups when analyzed by VUR grading or by VUR laterality. Multiregression analysis indicated that grade III VUR was a significant risk factor for repeat UTI (p < 0.01).
© 2013 2minutemedicine.com. All rights reserved. No works may be reproduced without expressed written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors, editors, staff or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT.





{kind=link}