
Treatment at lower glucose threshold noninferior to traditional threshold in newborns with asymptomatic hypoglycemia
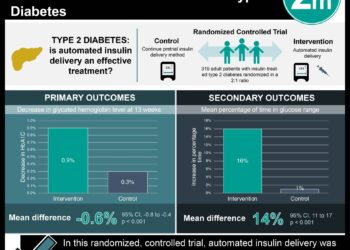
1. In this randomized noninferiority trial involving newborns with asymptomatic moderate hypoglycemia, initiation of treatment at a lower blood glucose threshold resulted in no significant difference in psychomotor development at 18 months versus the traditional threshold.
2. Fewer hypoglycemic episodes occurred in the traditional threshold group, although more invasive interventions were also performed. Recurrent hypoglycemia did not appear to affect psychomotor outcome, but further research must be done to exclude this possibility.
Evidence Rating Level: 2 (Good)
Study Rundown: Fluctuations in blood glucose can cause neurological damage, but an optimal management strategy has not yet been determined for neonatal hypoglycemia. Because of this ambiguity, operational protocols differ widely among care facilities, and both undertreatment and overtreatment are possible. While the traditional threshold for treatment is set at 47 mg per deciliter, it is hypothesized that a concentration between 36 mg per deciliter at 46 mg per deciliter is acceptable for brief periods. This study compared these two thresholds in four high-risk subgroups of healthy newborns, finding that Bayley-III-NL psychomotor development scores were similar between groups at 18 months. No correlation was detected between Bayley score and the number or severity of hypoglycemic episodes, and no infants with hypoglycemia exhibited any clinical symptoms. Two serious adverse events occurred in the lower threshold group, but neither was related to the treatment regimen. One limitation of this study was that the sample size was too small and homogenous to conclusively exclude the effects of recurrent hypoglycemia and that the results had weak generalizability. In light of this uncertainty, newborns at greater risk of hypoglycemia should maintain a higher target glucose concentration.
Click here to read the study in NEJM
Relevant Reading: Association of Neonatal Glycemia With Neurodevelopmental Outcomes at 4.5 Years
In-Depth [randomized controlled trial]: In this multicenter randomized trial, 689 neonates who were at risk for hypoglycemia were stratified according to subgroup and randomly assigned in a 1:1 ratio to receive treatment either when the glucose concentration was lower than 36 mg per deciliter or when the glucose concentration was lower than 47 mg per deciliter. The four at-risk subgroups were late-preterm infants (gestational age from 35 to 37 weeks), infants who were small (below the 10th percentile) or large (above the 90th percentile) for gestational age, and infants of mothers with diabetes. Treatment consisted of a 1 to 2 mg increase in carbohydrate intake per kilogram of bodyweight per minute. Noninferiority was defined as a difference of less than one half of one standard deviation (SD) in the average score on the Bayley Scales of Infant and Toddler Development. This inferiority limit was not crossed, and there was no significant difference between groups in the percentage of children with Bayley scores below -1 or -2 SD. In addition, both groups had similar durations of hospital stay and health care costs. Hypoglycemia occurred in 10% more of the newborns in the lower-threshold group than in the traditional-threshold group (95% confidence interval, 2 to 17 percentage points) but did not appear to affect psychomotor outcomes.
Image: PD
©2020 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.





{kind=link}