
#VisualAbstract: Double sequential external defibrillation and vector-change defibrillation improve outcomes in patients with refractory ventricular fibrillation
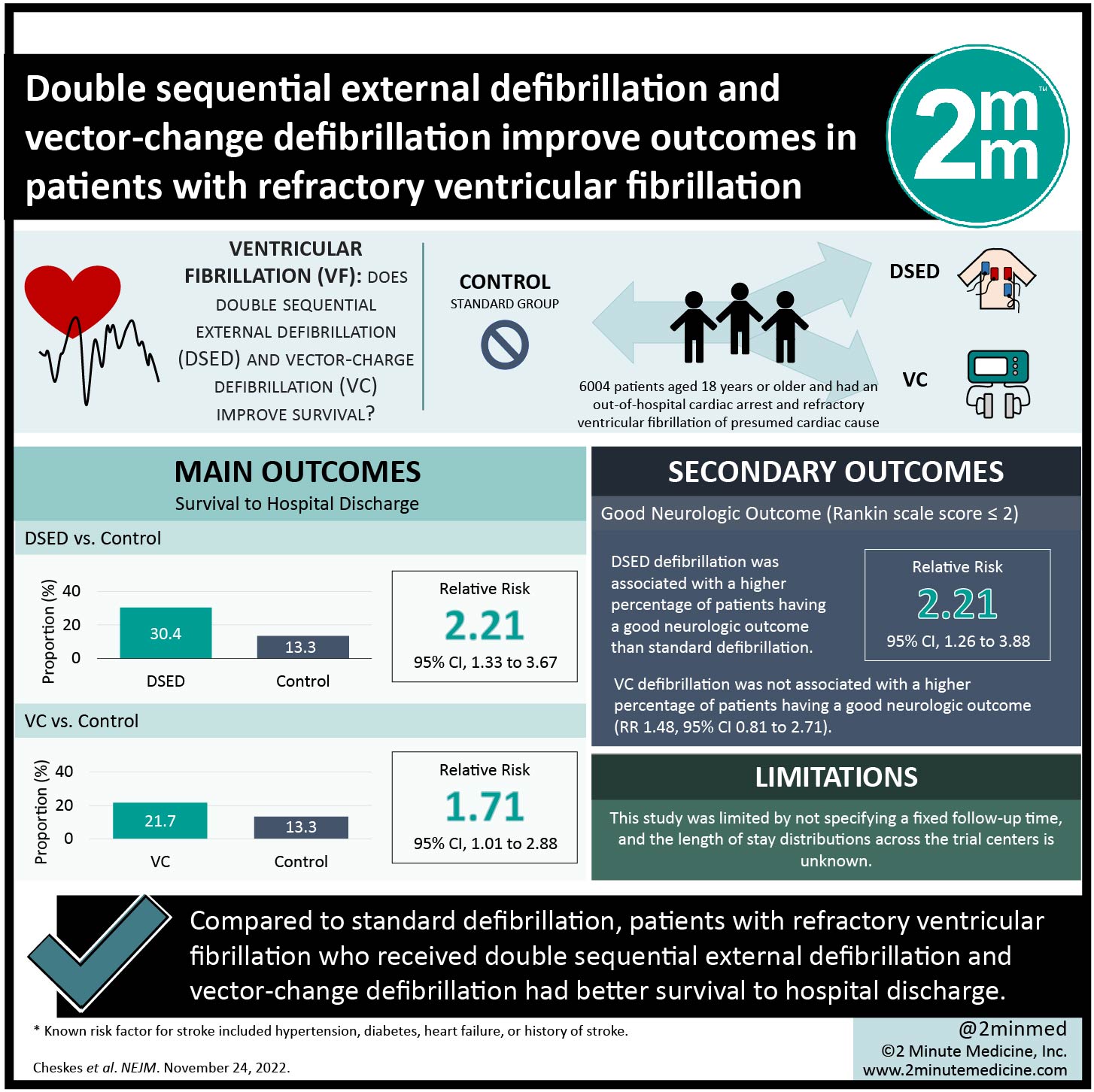 1. Compared to standard defibrillation, patients with refractory ventricular fibrillation who received double sequential external defibrillation (DSED) and vector-change defibrillation (VC) had better survival to hospital discharge.
1. Compared to standard defibrillation, patients with refractory ventricular fibrillation who received double sequential external defibrillation (DSED) and vector-change defibrillation (VC) had better survival to hospital discharge.
2. DSED was associated with a higher percentage of patients having a good neurologic outcome as compared to standard defibrillation.
Evidence Rating Level: 1 (Excellent)
Study Rundown: There are over 350,000 unexpected deaths each year in North America due to out-of-hospital cardiac arrest, with 100,000 of these cases attributed to ventricular fibrillation or pulseless ventricular tachycardia. Almost half of these patients may remain in refractory ventricular fibrillation despite multiple defibrillation attempts. DSED and VC have been proposed to provide potential benefits in defibrillating a portion of the ventricle that may not be completely defibrillated by pads in the standard anterior-lateral position. However, there is a gap in knowledge regarding the effectiveness of DSED and VC defibrillation compared with standard defibrillation in patients who remain in refractory ventricular fibrillation during out-of-hospital cardiac arrest. Overall, this study found that survival to hospital discharge was higher with DSED and VC defibrillation as compared to standard defibrillation in patients with refractory ventricular fibrillation. This study was limited by not specifying a fixed follow-up time, and the length of stay distributions across the trial centers is unknown. Nevertheless, the study’s findings are significant, as they demonstrate that DSED and VC defibrillation provide a higher survival to hospital discharge among patients with refractory ventricular fibrillation during out-of-hospital cardiac arrest.
Click to read the study in NEJM
Relevant Reading: Long-Term Outcomes of Out-of-Hospital Cardiac Arrest after Successful Early Defibrillation
In-Depth [cluster randomized trial]: This three-group, cluster-randomized, controlled trial with crossover was conducted in six paramedic services in Canada from March 2018 to May 2022. Patients who were at least 18 years of age and had an out-of-hospital cardiac arrest and refractory ventricular fibrillation of presumed cardiac cause were eligible for the study. Patients who had a traumatic cardiac arrest, do-not-resuscitate medical directives, or cardiac arrest due to drowning, hypothermia, hanging, or suspected drug overdose were excluded from the study. The primary outcome measure was survival to hospital discharge. Outcomes in the primary analysis were assessed via adjusted relative risks with generalized linear models with log link and binomial distribution. Based on the primary analysis, survival to hospital discharge was more common in the DSED group than in the standard group (30.4% vs. 13.3%; Relative Risk [RR], 2.21; 95% Confidence Interval [CI], 1.33 to 3.67) and more common in the VC group than in the standard group (21.7% vs. 13.3%; RR, 1.71; 95% CI, 1.01 to 2.88). DSED defibrillation was associated with a higher percentage of patients having a good neurologic outcome than standard defibrillation (RR, 2.21; 95% CI, 1.26 to 3.88). Overall, this study demonstrated that for patients with refractory ventricular fibrillation, survival to hospital discharge occurred more frequently in those who received DSED or VC defibrillation than those who received standard defibrillation.
©2022 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports





{kind=link}
