
#VisualAbstract: Dual therapy with infliximab and IVIG in children with multi-system inflammatory syndrome
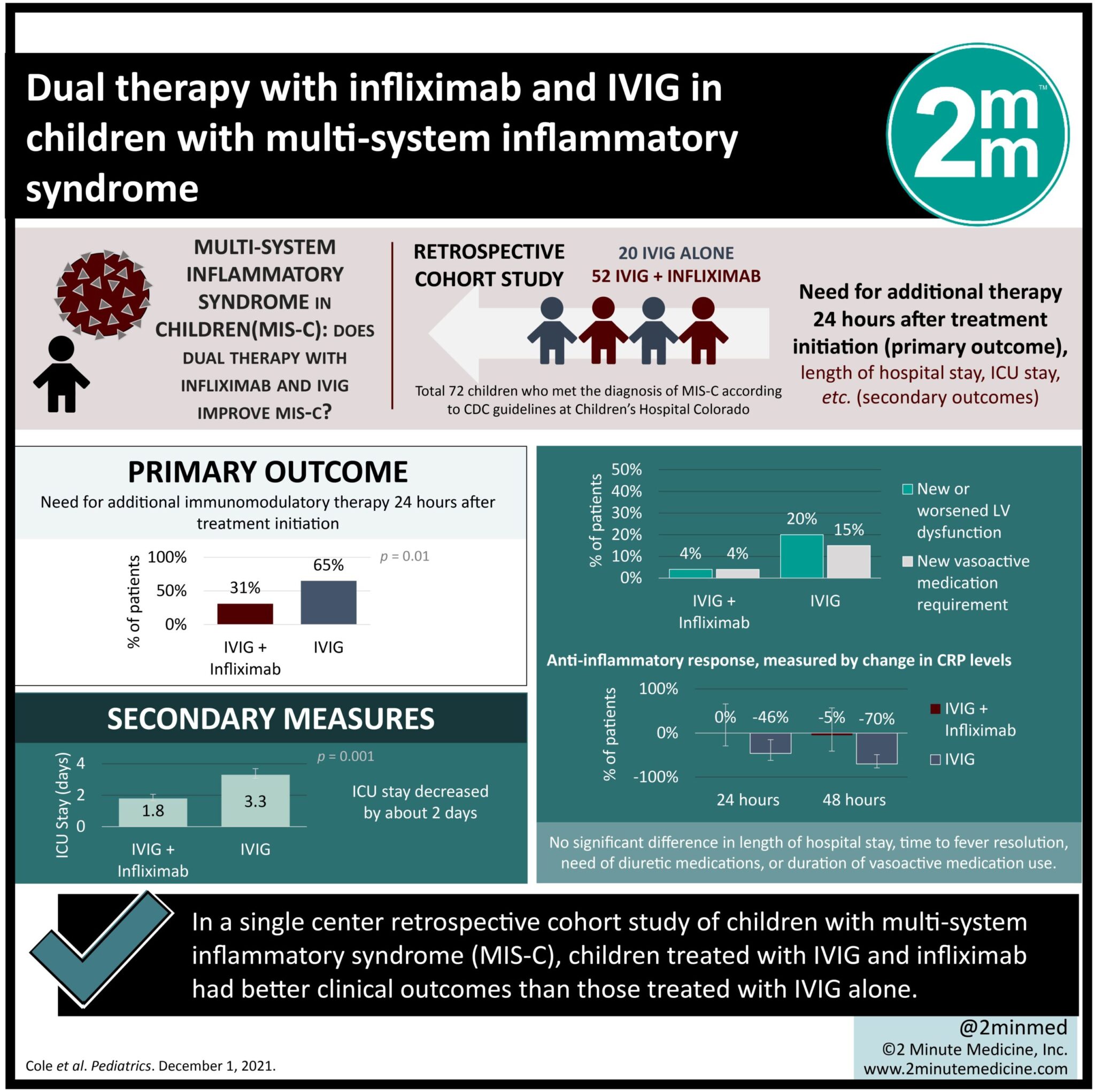
1. In a single center retrospective cohort study of children with multi-system inflammatory syndrome (MIS-C), children treated with IVIG and infliximab had better clinical outcomes than those treated with IVIG alone.
2. Children who received infliximab had better cardiac outcomes, had a shorter ICU stay, and showed more rapid decline in inflammation.
Evidence level: 2 (Good)
Study Rundown: One clinical sequalae of pediatric COVID-19 infection is the development of multi-system inflammatory syndrome in children (MIS-C), a highly inflammatory state that can lead to end-organ damage and even death. The use of intravenous globulin (IVIG) is the standard of care in treating these patients, but the addition of biologic therapies has not been well-studied. This single-center retrospective study from Colorado aimed to assess the value of dual therapy with infliximab and IVIG in iproving clinical outcomes in MIS-C compared to IVIG alone. Results showed that fewer patients on dual therapy required additional medical therapy 24 hours later (31%) than with single therapy (65%); patients’ stay in the ICU was decreased by 2 days; and fewer patients developed left ventricular dysfunction (LV) with dual therapy (3%) versus 19% with IVIG alone. A major strength of this study is that it includes patients who met the CDC criteria for the disease, allowing it to be easily replicated at other centers. However, the retrospective study design is a major limitation in ruling out contributing confounding factors, and randomized controlled trials are still necessary. Overall, this study indicates that improved clinical outcomes may be associated with the addition of infliximab to IVIG in the treatment of MIS-C.
Click here to read the original article
Relevant reading: SARS-CoV-2-associated multisystem inflammatory syndrome in children: clinical manifestation and the role of infliximab treatment
In-depth [retrospective cohort]: This is a single center retrospective cohort study from Children’s Hospital Colorado analyzing data between April 1 and February 28, 2021. During this time, 72 children were diagnosed with MIS-C in accordance with the CDC criteria. The primary variable of interest was the need for additional immunomodulatory therapy 24 hours after initial therapy. Secondary outcomes included length of ICU stay, new or worsening LV dysfunction, need for diuretics, and decreased inflammation. Children treated with dual therapy of IVIG (2 g/kg given over 10-12 to 20-24 hrs) and Infliximab (10 mg/kg) compared to IVIG alone less frequently required additional therapy (16 of 52 [31%] vs. 13 of 20 [65%]); had a lower rate of new or worsening LV dysfunction (3% vs. 19%); and had a more pronounced anti-inflammatory response as measured by decline in CRP levels (-70% vs. -5%) 48 hours post-treatment. No significant difference was found in the length of hospital stay, time to fever cessation, vasoactive medication duration, or the need for diuretics. Infliximab-followed-by-IVIG had better outcomes in the need for diuretics compared to IVIG-followed-by-infliximab (29% vs. 75%) and led to a sharper decline in CRP levels (-54% vs. -16%) 24 hours post-treatment. However, no differences in cardiac outcomes were found for either treatment sequence.
Image: PD ©2021 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports






{kind=link}
