




{kind=link}


2 Minute Medicine Rewind January 13, 2020
1. There is a significantly increased risk of dementia in patients with previously diagnosed depression, with the highest risk observed in patients diagnosed with severe depression
Evidence Level: 2 (Good)
The prevalence of dementia is on the rise. With a scarcity of effective treatment options, increased emphasis has been placed on the identification of risk factors and effective prevention of the disease. Depression has previously been found to be associated with greater dementia risk, though the pre-existing literature examining the relationship between the two conditions has been inconclusive. Specifically, previous research has been characterized by short follow up times, making it unclear as to whether there was a true association, or if depression could be manifesting as a prodromal phase or early indicator of dementia. To address this knowledge gap, researchers of the present study sought to better characterize the relationship between the two conditions by performing a nationwide cohort study using the data between 1964 through 2016 from the Swedish National Patient Register. The study consisted of a cohort of individuals diagnosed with depression (n=119,386) with matched controls without depression diagnosis and a second cohort of siblings (n=50,644) consisting of same-sex full sibling pairs with discordant depression status. Researchers found an increased risk of dementia in the population matched cohort study, with 9802 individuals being diagnosed with dementia during a mean follow-up period of 10.41 years (OR 2.47, 95% CI 2.35 to 2.58, p<0.001). In examining specific diagnoses, researchers noted even stronger associations between depression and vascular dementia (OR 2.68, 95% CI 2.44 to 2.95, p<0.001) and Alzheimer’s disease (OR 1.79, 95% CI 1.68 to 1.92). The association was strongest within the first 6 months after depression diagnosis (OR 15.20, 95% CI 11.85 to 19.50, p<0.001), and remained significant even 20 years after follow-up (OR 1.58, 95% CI 1.27 to 1.98, p<0.001). Similar findings were elicited in the sibling cohort study, suggesting that the association exists despite accounting for some familial factors. This study therefore shows that, although a causal relationship cannot be established, there is a positive, enduring relationship between depression and dementia. In addition to risk identification, these findings also warrant investigation of successful prevention and treatment of depression as a means of decreasing dementia risk.
Early surgery or conservative care for asymptomatic aortic stenosis
1. Patients with asymptomatic severe aortic stenosis receiving early valve replacement had a lower incidence of operative mortality or death due to cardiovascular causes compared to patients receiving conservative care
Evidence Level: 1 (Excellent)
Aortic stenosis is the most common valvular disease with surgical indications in developed countries, with aortic-valve replacement being the only effective treatment option for severe symptomatic stenosis. Currently, the consensus opinion is to reserve surgical intervention for patients with symptomatic severe aortic stenosis, with observation and conservative management for asymptomatic patients. In asymptomatic patients, surgical risks have been largely regarded as outweighing the potential benefits of valve replacement. Advancements in surgical techniques, technology, and postoperative care, however, have raised questions surrounding the safety of performing valve replacement earlier in asymptomatic patients. In this multicenter, randomized controlled trial, 145 asymptomatic patients with very severe aortic stenosis (aortic-valve area of ≤0.75 cm2 with either an aortic jet velocity of ≥4.5 m per second or a mean transaortic gradient of ≥50 mm Hg) between July 2010 through April 2015 to either undergo early surgery group or receive conservative care. The primary end point was a composite of operative mortality, consisting of death during or within 30 days of surgery, or death from cardiovascular causes during the entire follow up period (median follow up 6.2 years). Researchers found there was no operative mortality found in the early intervention group, and, in an intention-to-treat analysis, the early treatment group had significantly fewer end events compared to the conservative treatment group (HR 0.09, 95% CI 0.01 to 0.67, p=0.003). The incidence of death due to any cause was also lower in the intervention group compared to the conservative treatment group. This study therefore supports earlier surgical intervention for asymptomatic patients with very severe aortic stenosis, with reduced operative risk possibly owing to improved surgical technique and postoperative care.
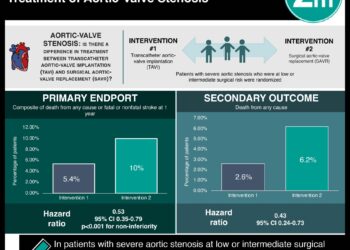
A controlled trial of rivaroxaban after transcatheter aortic-valve replacement
1. After successful transcatheter aortic valve replacement, compared to an anti-platelet based strategy, patients that received an anti-coagulation strategy including rivaroxaban at a dose of 10 mg daily had a higher risk of death, thromboembolic complications, and bleeding.
Evidence Rating: 1 (Excellent)
Transcatheter aortic-valve replacement (TAVR) is a treatment option for patients with severe symptomatic aortic stenosis. Currently, guidelines recommend dual antiplatelet therapy following successful TAVR to prevent thromboembolic events (TE) and complications such as stroke, MI, and DVT. Although rivaroxaban, a factor Xa inhibitor, has been shown to reduce TE events in other clinical settings, its suitability for post-TAVR anticoagulation has not been well studied. In this randomized controlled trial, 1644 patients without an absolute contraindication to anticoagulation or absolute indication for antiplatelet therapy were assigned to receive either anticoagulation (rivaroxaban 10 mg daily plus aspirin 75-100 mg daily for 3 months, followed by rivaroxaban monotherapy 10 mg) or dual antiplatelet therapy (aspirin 75-100 mg daily plus clopidogrel 75 mg daily for 3 months followed by aspirin monotherapy 75-100 mg). The primary efficacy outcome of interest was death or TE events, and the primary safety outcome was major bleeding events. After a median follow-up of 17 months, researchers found that there were significantly greater deaths or major TE events in the rivaroxaban group (HR 1.35, 95% confidence ratio 1.01 to 1.81, p=0.04) compared to the antiplatelet group. Deaths from any cause were also higher in the anticoagulant group (HR 1.69, 95% CI 1.13 to 2.53) when compared to the antiplatelet group. Based on an intention to treat analysis there were also a greater number of major, disabling, or life-threatening bleeding events in the anticoagulant group (HR, 1.50, 95% CI 0.95 to 2.37, p=0.08), though these results did not reach statistical significance. Overall, the results of this study do not support anticoagulant therapy with rivaroxaban 10 mg daily as a noninferior alternative to the currently recommended dual antiplatelet therapy post TAVR, given its increased risk of both TE events and bleeding related complications.
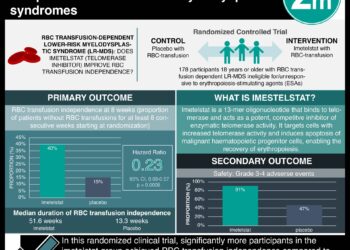
Luspatercept in Patients with Lower-Risk Myelodysplastic Syndromes
1. Luspatercept may significantly reduce transfusion burden in patients with lower-risk myelodysplastic syndromes with ring sideroblasts for whom erythropoiesis-stimulating agents have not been effective
Evidence Rating: 1 (Excellent)
Myelodysplastic syndromes are acquired bone marrow disorders characterized by ineffective hematopoiesis, progressive cytopenias and an increased risk of acute myeloid leukemia, predominantly seen in the elderly population. Lower risk myeodysplastic syndromes most commonly manifest as symptomatic anemia, and are associated with cardiovascular complications, falls, and shorter survival. A large proportion of these patients eventually become dependent on red-cell transfusions, which are associated with reduced quality of life and overall survival. Currently, erythropoiesis-stimulating agents are first-line treatments for lower-risk myelodysplastic syndromes, and are used to increase the duration of transfusion independence. Alternative treatment options are limited to use in certain patient populations such as patients with myelodysplastic syndromes with ring sideroblasts, who tend to remain responsive to stimulating agents for shorter durations of time. In this double-blind, placebo-controlled, phase 3 trial, 229 patients with very-low risk, low-risk or intermediate-risk myelodysplastic syndrome with sideroblasts who had been receiving regular red-call transfusions were randomized to receive luspatercept (1.0 to 1.75 mg/kg) or placebo administered subcutaneously every 3 weeks to study the efficacy of luspatercept as a novel treatment option, with transfusion independence being the primary end point. Researchers found that patients assigned to receive luspatercept had a significantly higher rate of transfusion independence for 8 weeks or longer (38%) compared to the placebo group (13%) during weeks 1 to 24 (p<0.001). Findings persisted with the experimental group having a higher likelihood of being transfusion independent at 12 weeks or longer through weeks 1 to 24 and 24 to 48 (p<0.001 for both comparisons). This study therefore shows that in patients with lower-risk myelodysplastic syndromes with ring sideroblasts, luspatercept may represent a promising treatment option where erythropoiesis-stimulating agent therapies are ineffective.
1. Smoking cessation without weight gain in patients with type 2 diabetes is associated with a lower risk of cardiovascular disease and all-cause and cause-specific mortality.
2. Weight gain after smoking cessation lessens the reduction in risk of experiencing cardiovascular events, emphasizing the importance of bodyweight control after cessation.
Evidence Rating: 2 (Good)
Lifestyle modifications, including smoking cessation, play an important role in the prevention and management of type 2 diabetes, and related macrovascular complications. Smoking cessation, however, is often accompanied by weight gain, raising concerns surrounding poorer diabetes control. In this prospective, population-based cohort study, data from the Nurses’ Health Study and Health Professionals Follow-up Study were used to investigate the association between cardiovascular disease and all-cause mortality with weight gain and smoking cessation in 10,809 patients with type 2 diabetes. Researchers found that recent quitters (2-6 consecutive years since smoking cessation) that did not have associated weight gain within this time period had a significantly lower risk of cardiovascular disease than patients who continued to smoke (HR 0.83, 95% CI 0.70 to 0.99) as well as recent quitters with a coinciding weight gain of 0.1 kg to 5 kg (HR 0.89, 95% CI 0.65 to 1.23), or more than 5 kg (HR 0.72, 95% CI 0.61 to 0.84). The findings of this study therefore reemphasize the importance of smoking cessation in reducing the risk of developing cardiovascular disease, morbidity and mortality. However, the importance of body weight management following cessation must also be communicated to patients, as associated weight gain can attenuate the positive effects of smoking cessation.
Image: PD
©2020 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.
RelatedReports
