
2 Minute Medicine Rewind September 9 – September 15, 2013
Image: PD
In this section, we will highlight the key high-impact studies, updates, and analyses published in medicine during the past week.
Pretreatment with Prasugrel in Non–ST-Segment Elevation Acute Coronary Syndromes
Prasugrel, a P2Y12 receptor antagonist anti-platelet medication, has been previously shown to be effective in treating non-ST-segment elevation (NSTE) acute coronary syndromes. However, the effect of administering the medication before versus after coronary angiography is unknown. In this randomized control trial of 4033 patients with NSTE acute coronary syndromes scheduled for coronary angiography, patients were randomized to receive either a 30 mg loading dose of prasugrel and an additional 30 mg of prasugrel at the time of percutaneous coronary intervention (PCI) or just 60 mg of prasugrel at the time of PCI. There was no statistical difference in the primary outcome of composite death from cardiovascular causes, myocardial infarction, stroke, urgent revascularization, or glycoprotein IIb/IIa inhibitor rescue therapy through day 7 (hazard ratio 1.02, 95% CI 0.84-1.25, p=0.81). However, there was a significantly increased rate of Thrombolysis in Myocardial Infarction (TIMI) major bleeding episodes (hazard ratio 1.90, 95% CI 1.19-3.02, P=0.006). This study therefore suggests that pre-treatment with prasugrel does not significantly reduce the rate of major ischemic events but instead increases the rate of major bleeding complications in patients with NSTE acute coronary syndrome undergoing coronary angiography.
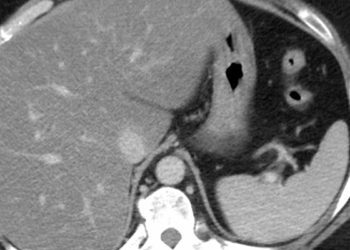
Alcoholic hepatitis continues to be an extremely challenging condition to treat with a substantial portion of patients dying at 6 months despite first line treatments. Prednisolone and pentoxifylline have each been shown in previous trials to improve survival, however using them in combination has yet to be thoroughly explored. In this randomized control trial, 270 patients with alcoholic hepatitis and a Maddrey score of at least 32 were assigned to receive either a combination of 40mg of prednisolone once a day and 400mg of pentoxifylline three times a day or 40 mg of prednisolone and a placebo for 28 days. At 6 months there was no statistical difference in survival between the two groups (69.9% (95% CI 62.1%-77.7%) vs 69.2% (95% CI 61.4%-76.9%), p=0.91). While it has been proposed that pentoxifylline may reduce the incidence of hepatorenal syndrome, there was no statistical difference in hepatorenal syndrome incidence between these two groups (8.4% (95% CI 4.8%-14.8%) vs. 15.3% (95% CI 10.3%-22.7%), p = 0.07), although the study may have been merely underpowered to detect a difference in this outcome. These results demonstrate that adding pentoxifylline to a 4-week regimen of prednisolone produces no apparent additional benefit in survival at 6 months in patients with alcoholic hepatitis.
With the Affordable Care Act, hospital systems will be implementing pay-for-performance programs. However, previous evidence for the effectiveness of such measures has been conflicting, with additional possible variation existing between programs that reward individual care providers versus health practice teams. In this cluster randomized trial, 12 Veterans Affairs outpatient clinics, with altogether 83 primary care physicians and 42 non-physician personnel, were assigned to receive either physician-level incentives, practice-level incentives, physician-level plus practice-level incentives, or no incentives for following hypertension practice guidelines over a period of 20 months. Average total payments by the end of the study were $4270, $2672, and $1648 for combined, individual, and practice-level incentive groups respectively. The baseline and final percentages in patients meeting blood pressure response measures were 75% to 84% (95% CI 4.20-11.80%) for the individual incentive group, 80% to 85% (95% CI 0.24-7.68%) for the practice-level incentive group, 79% to 88% (95% CI 1.92-9.52%) for the combined group, and 86% to 86% (95% CI −3.12-4.04%) for the control group. The only group that showed a statistically significant difference from the control group in the proportion of patients meeting blood pressure control measures was the individual incentive group, which demonstrated an 8.63% increase (95% CI 2.40-13.00%, p=0.005). None of the incentive groups demonstrated increased use of guideline-recommended medications or incidence of hypotension when compared with controls. This study shows that individual financial incentives for following hypertension guidelines, but not practice-level or combined incentives, resulted in improved blood pressure control compared with controls.
Gonadal Steroids and Body Composition, Strength, and Sexual Function in Men
Testosterone therapy is growing in popularity among men, however currently there is no rigorous clinical characterization of testosterone deficiency with most testosterone prescriptions prescribed for a combination of vague symptoms such as fatigue or sexual dysfunction when seen in the setting of low testosterone lab levels. In this two-cohort, randomized control trial, 400 participants aged 20-50 years old were given goserelin acetate every 4 weeks over 12 weeks to suppress endogenous gonadal steroids. Patients in cohort one were randomly assigned to receive placebo, 1.25 g, 2.5 g, 5 g, or 10 g of topical 1% testosterone gel for 16 weeks. Patients in cohort 2 were additionally given anastrozole to block the aromatization of testosterone to estrogen. Investigators found that the percentage of body fat increased significantly in groups receiving 2.5 g of testosterone daily or less in cohort one and across all groups in cohort two, suggesting an independent effect of estradiol. Lean mass and thigh-muscle area also decreased significantly in groups receiving 1.25 g of testosterone daily or less in cohort one and only in the placebo group in cohort two. In both cohorts, leg-press strength decreased significantly only in men receiving placebo and sexual desire decreased with lower testosterone doses. Overall, this study demonstrated that the amount of testosterone required to maintain lean mass, fat mass, strength, and sexual function can vary substantially and that in general androgen deficiency results in decreases in lean mass, muscle area, and strength whereas estrogen deficiency causes increases in body fat. Both androgen and estrogen deficiency caused reduced sexual function.
Electronic cigarettes for smoking cessation: a randomised controlled trial
Electronic cigarettes (e-cigarettes) are becoming popular nicotine delivery devices and have been proposed as a method for assisting with smoking cessation. In this randomized control trial, 657 patients in New Zealand were randomized to nicotine e-cigarettes, nicotine patches, or placebo e-cigarettes for smoking cessation. At 6 months, the proportion of nicotine abstinent patients was 7.3% with nicotine e-cigarettes, 5.8% with patches, and 4.1% with placebo e-cigarettes. The risk difference for nicotine e-cigarettes compared to patches was 1.51 (95% CI -2.49-5.51) and compared to placebo e-cigarettes was 3.16 (95% CI -2.29-8.61). This study underestimated the rates of abstinence and was therefore underpowered to show statistically significant superiority of nicotine e-cigarettes. Nevertheless, it was shown that e-cigarettes could achieve similar levels of abstinence as nicotine patches.
Approximately 60% of Type 2 diabetics will achieve remission after Roux-en-Y gastric bypass (RYGB) surgery, however to-date there has been no accurate method for predicting pre-operatively the probability of such remission. In this retrospective cohort study, investigators studied a cohort of 690 patients who underwent RYGB surgery and created multiple logistic regression models with 259 clinical variables to identify independent predictors of remission, defined as lasting for more than 1 year. The study found that the strongest predictors for remission were insulin use, age, HbA1c concentration, and type of antidiabetic drugs used. The investigators then produced the “DiaRem” score (with a range of 0-22) utilizing these 4 variables with Kaplan-Meier analysis showing that 88% (95% CI 83-92%) of patients who scored 0-2, 64% (58-71%) who scored 3-7, 23% (13-33%) who scored 8-12, 11% (6-16%) who scored 13-17, and 2% (0-5%) of those who scored 18-22 achieved early remission. The DiaRem score is the first preoperative method for predicting the probability of type 2 diabetes remission after RYGB surgery.
By Neal Yuan and David Ouyang
© 2013 2minutemedicine.com. All rights reserved. No works may be reproduced without written consent from 2minutemedicine.com. Disclaimer: We present factual information directly from peer reviewed medical journals. No post should be construed as medical advice and is not intended as such by the authors or by 2minutemedicine.com. PLEASE SEE A HEALTHCARE PROVIDER IN YOUR AREA IF YOU SEEK MEDICAL ADVICE OF ANY SORT. Content is produced in accordance with fair use copyrights solely and strictly for the purpose of teaching, news and criticism. No benefit, monetary or otherwise, is realized by any participants or the owner of this domain.





{kind=link}