
The 2 Minute Medicine Podcast Episode 18
June 29th 2023
Welcome to the 2 Minute Medicine Podcast, summarizing the latest medical studies, curated and written by practicing physicians. On this podcast, twice a month, we cover the latest in healthcare news and research evidence.
Our episode is live!
Episode Description
We begin this episode by discussing our article of the week from the New England Journal of Medicine entitled “Hydrocortisone in severe community-acquired pneumonia.“. In the second half of our episode, we bring a medical eye to popular events. We begin with a discussion about how the federal drug administration recently approved a drug to treat some symptoms of menopause. Then we take a closer look at the affordable care act mandate for preventative care. Last, but not least, we have a conversation about pride month and inequalities that exist in the healthcare system for the LGBTQ+ community and Nirsevimab, an antibody that can help prevent severe symptoms of RSV in infants!
Click here to listen to this episode on Apple podcast
Click here to listen to this episode on Spotify
Transcript
[Deepti] Welcome to the 2 Minute Medicine Podcast, summarizing the latest medical studies, curated and written by practicing physicians.
For our full suite of daily medical study summaries and updates written by practicing doctors, please visit our website at 2minutemedicine.com to start reading new daily content right now, for free. On this podcast, twice a month, we cover the latest in health care news and research evidence. We are your hosts Deepti and Andrew. On today’s episode, we’ll start off by discussing our two articles of the week. In the second half of the episode, we will look at health issues that have arisen in popular media.
[Andrew] Our article of the week comes from the New England Journal of Medicine and is entitled “Hydrocortisone in severe community-acquired pneumonia.”
Community-acquired pneumonia (CAP) is a prevalent lower respiratory infection affecting millions of individuals worldwide on an annual basis. The death rates of hospitalized and ICU patients with CAP remain significant despite advancements in care. Notably, the pathophysiology of pneumonia-related morbidities and mortality involves severe inflammation. Therefore, glucocorticoids have been investigated as a potential treatment for these patient populations. Despite some clinical benefits, mortality benefits have not been established.
The current study was a randomized controlled trial assessing the impact of hydrocortisone on the clinical status of adult patients admitted to the ICU for severe CAP. The severity of pneumonia was defined as the presence of at least one of mechanical ventilation, high-flow oxygen administration, nonrebreathing mask usage, or a score ≥130 on the Pulmonary Severity Index. Exclusion criteria included a do-not-intubate order, influenza-related pneumonia, and septic shock. The primary outcome was all-cause mortality by day 28.
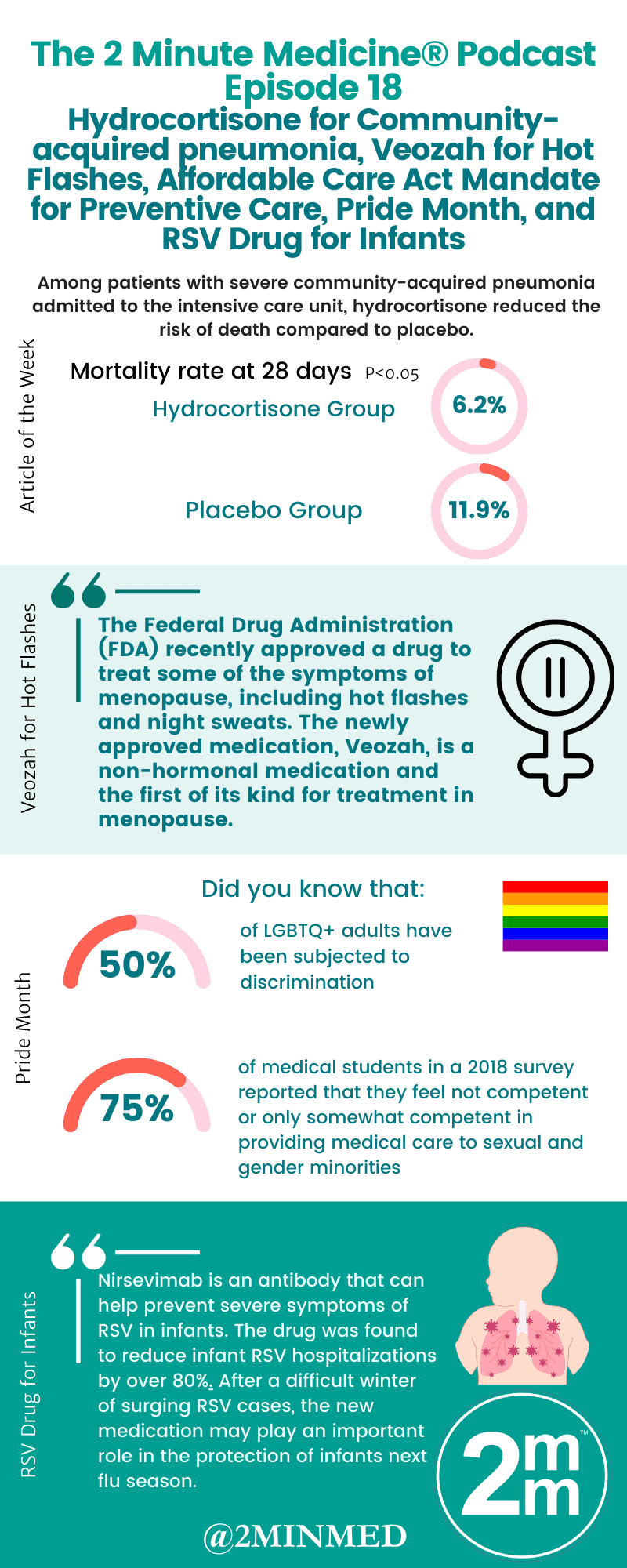
Overall, 800 patients were randomized to receive intravenous hydrocortisone 200mg daily as guided by clinical improvement or a placebo. By 28 days, the mortality rate was 6.2% in the hydrocortisone group and 11.9% in the placebo group (absolute difference -5.6 percentage points; 95% Confidence Interval [CI], -9.6 to -1.7; p=006). The rate of endotracheal intubation among those not receiving mechanical ventilation at baseline was lower in the hydrocortisone group compared to placebo (hazard ratio [HR], 0.59; 95% CI, 0.40 to 0.86). Similarly, the rate of vasopressor initiation was lower in the hydrocortisone group (HR, 0.59; 95% CI, 0.40 to 0.86). The rates of serious adverse events, ICU-acquired infections, and gastrointestinal bleeding were comparable between the two groups. However, in the first week of therapy, hydrocortisone recipients received a higher median daily insulin dose than those receiving placebo.
In summary, these results demonstrated a mortality benefit of early treatment with hydrocortisone among adults admitted to the ICU with severe CAP. The study was limited by the low observed mortality in the control group, the exclusion of septic shock patients, and a low number of immunocompromised patients. Nevertheless, these results demonstrated a clear 28-day mortality benefit of hydrocortisone for ICU patients with severe CAP. The study was discontinued at the second planned interim analysis.
[Andrew] Now for the Scan by 2 Minute Medicine®, a pop-culture medical newsletter and exclusive benefit for 2 Minute Medicine Plus subscribers. We will start off by talking about menopause.
The Story: The Federal Drug Administration (FDA) recently approved a drug to treat some of the symptoms of menopause, including hot flashes and night sweats. The newly approved medication, Veozah, is a non-hormonal medication and the first of its kind for treatment in menopause. The new treatment option represents an exciting new development, especially for those who are unable to take standard hormonal therapies.
Before we delve deeper into managing its symptoms, let’s take a closer look at what the symptoms of menopause could be. Menopause is the changes that occur in middle age women that involve the end of menstrual periods. Menopause typically occurs anywhere between the ages of 45 and 55 and is defined as the 12 months following a woman’s last menstrual period. Although it is only these 12 months that define menopause, the menopausal transition, or perimenopause, which includes the onset of irregularities in menstrual cycles and symptoms, can last several years. Common symptoms of menopause are due to fluctuations in estrogen levels and can include changes in sexual function, mood swings, hot flashes, and night sweats. Although menopause is a normal part of life, there is a lot of stigma around the transition, with many women experiencing shame and embarrassment. In fact, a UK study showed that nearly half of menopausal women haven’t spoken to their doctor about menopausal symptoms because of the stigma. These feelings towards menopause affect the workplace as well, with studies showing that many women feel they need to suffer silently at work. As a result, there is a push for “menopause-friendly” workplaces which educate workers about the stigma and employ policies that make the transition easier for women. Talking about menopause and recognizing it as a normal part of life can help reduce the social burden that is placed on women going through this transition.
[Deepti] That’s right! Managing menopause symptoms can also be a challenge. Studies show that nearly three quarters of menopausal women don’t seek treatment for their symptoms. Not only can poor symptom management lead to discomfort, but it can also have health implications. Studies show that an increased frequency of symptoms such as hot flashes and night sweats is correlated with weight gain, poorer cardiovascular health scores, and lower overall quality of life. The typical treatment for these symptoms is hormone therapy: either estrogen alone or in combination with progesterone. These treatments are quite effective, but for those who are unable to use these therapies, such as past and present hormone-sensitive breast cancer patients, the options are quite limited. The new drug, Veozah will hopefully serve as an important alternative to manage symptoms in those who are unable to take standard therapies.
Now let’s take a closer look at the affordable care act mandate for preventive care.
The part of the Affordable Care Act that requires insurance companies to cover the cost of preventive care has been restored after some uncertainty. Earlier this year, the mandate was ruled as unconstitutional in court, which put access to many preventive care options for Americans in jeopardy. However, deliberations on whether to remove this part of the act are ongoing.
Preventive medicine is the branch of medicine involved in preventing or stopping disease. Preventive medicine is often seen as the gold standard: making sure people don’t get sick, rather than treating them once they have already fallen ill. Things that fall under the umbrella of preventive medicine include cancer screening, HIV prevention with the pre-exposure prophylaxis (PrEP) pill, vaccinations, and more. These interventions are often very successful, with the PrEP pill alone reducing the risk of sexual transmission of HIV by nearly 99%.
[Andrew] Just to add to this, not only does preventive medicine result in improved patient outcomes, but it also has a huge economic benefit. With so much money diverted to the management of chronic disease, estimates suggest that finding and treating conditions early could result in significant cost savings. Unfortunately, if insurance companies are no longer required to pay for these preventive measures, they will become inaccessible for many Americans.
Next, let’s talk about Pride Month, a time to celebrate the LGBTQ+ community! It is also a time to draw attention to the inequalities that exist in this community and advocate for equality. With regard to the healthcare system, LGBTQ+ folks face unique challenges. For example, LGBTQ+ youth are at higher risk for several conditions, including sexually transmitted infections, cancers, mental health struggles, and more. LGBTQ+ folks are also less likely to have a primary care provider, and youth in this community are less likely to access necessary medical care than non-LGBTQ+ youth. As a result, the LGBTQ+ community experiences worse health outcomes than the general population.
[Deepti] One of the reasons for these findings is because of discrimination and stigma. Studies show that over 50% of surveyed LGBTQ+ adults have been subjected to discrimination, and this is also prevalent in the healthcare system. Part of this stems from a lack of education: more than three-quarters of medical school students in a 2018 survey reported that they feel not competent or only somewhat competent in providing medical care to sexual and gender minorities. Although medical school teaching on LGBTQ+ health is limited, some schools are focusing on including more of this teaching into their curriculum. Developing cultural competency in treating LGBTQ+ patients is one way to ensure the medical system is a safe space for all.
Last but not least, let’s take a closer look at an RSV. Following a significant spike in respiratory syncytial virus (RSV) over the winter, an advisory committee for the FDA unanimously voted in favor of approving a drug to protect infants against RSV. If the FDA follows the advice of the advisory panel and approves the drug, Nirsevimab would be the first to protect infants from RSV. RSV typically presents as an upper respiratory tract infection but can also infect the lower respiratory tract. Although very common, serious illnesses can ensue in infants. In fact, RSV is one of the most common causes of death in the first year of life globally, second only to malaria. This is because infection can lead to a number of complications, including pneumonia. Although RSV can infect someone at any age, infants are more susceptible to harmful effects because of their reduced exposure and immunity. Furthermore, RSV leads to an inflammation of the airways.
[Andrew] Infants have smaller airways and are more susceptible to this inflammation, leading to more significant symptoms. As a result, there is a huge push to protect infants from the potentially harmful effects of RSV. The drug up for debate, Nirsevimab, is an antibody that can help prevent severe symptoms of RSV in infants. The drug was found to reduce infant RSV hospitalizations by over 80%. After a difficult winter of surging RSV cases, the new medication may play an important role in the protection of infants next flu season.
We’d like to acknowledge the following members of our team for their contributions to this week’s episode
- Benjamin Lam
- Kiera Liblik
- Ashley Jackson
Thank you for joining us today for this episode of the 2 Minute Medicine Podcast. New episodes come out every other week and all of our content has been curated and written by practicing physicians.

Please head to our website at 2minutemedicine.com to learn more and to access all of our content including medical study summaries, visual abstracts, excerpts from our Classics book series which is available on Amazon, and The Scan, which is our medical newsletter.
Thank you so much once again. To make sure that you don’t miss any of our content please subscribe and follow us on Twitter or Instagram @2MinMed
©2023 2 Minute Medicine, Inc. All rights reserved. No works may be reproduced without expressed written consent from 2 Minute Medicine, Inc. Inquire about licensing here. No article should be construed as medical advice and is not intended as such by the authors or by 2 Minute Medicine, Inc.






{kind=link}